The main difference between PHP and IOP is time and intensity. PHP usually involves 20 to 35 hours of treatment per week, often 5 to 7 days a week for 4 to 6 hours a day, while IOP usually involves 9 to 20 hours per week, often 3 to 5 days a week for 2 to 4 hours a day.
If you're reading this, you're probably doing what many families do in a hard moment. You're searching late at night, comparing program names, trying to figure out what fits your loved one, and getting buried in acronyms that all sound important but not very clear.
A parent may be asking, "Does my daughter need more structure than weekly therapy?" A spouse may be wondering, "Can he still work if he starts treatment?" And many people land on the same question: what is the difference between IOP and PHP, and how do you know which one is the safer choice?
The confusing part is that these programs can sound similar because both are outpatient care. The important part is that they serve different needs. One offers a near full-time treatment schedule with more oversight. The other offers structured care that fits around daily life when a person can stay stable between sessions.
There's also a part families often miss. More treatment hours don't always mean more safety if the person goes home each night to stress, conflict, substance use, or other strong triggers. That home piece matters more than many comparison pages acknowledge.
Table of Contents
- Navigating Your Mental Health Treatment Options
- PHP vs IOP At a Glance
- A Deep Dive into Partial Hospitalization Programs PHP
- A Deep Dive into Intensive Outpatient Programs IOP
- How to Decide Which Program Is Right for You
- Navigating Insurance Costs and Care at Casa Recovery
- Frequently Asked Questions About PHP and IOP
- Can someone start in PHP and later move to IOP
- Can someone move back up from IOP to PHP
- Is IOP enough if someone is still struggling
- Does PHP mean inpatient treatment
- Are families involved in treatment
- Which is better for dual diagnosis
- How long do PHP and IOP last
- What should I ask on an intake call
Navigating Your Mental Health Treatment Options
A common intake call starts like this: "We've looked at three websites, and now we're more confused than when we started." That reaction makes sense. PHP, IOP, outpatient, dual diagnosis, medication management, trauma-informed care. These terms can feel clinical and distant when what you really want is a simple answer about what kind of help your family member needs right now.
Think of treatment levels like different amounts of scaffolding around a building under repair. Some people need more support around them each day while things are fragile. Others are ready for less scaffolding because they can hold steady between appointments and practice skills in everyday life.
What these programs are in plain language
A Partial Hospitalization Program, or PHP, is a higher-structure daytime program. A person attends treatment for a large part of the day and then goes home in the evening.
An Intensive Outpatient Program, or IOP, is a lower-structure outpatient option. A person still receives consistent care, but the schedule leaves room for work, school, parenting, or other responsibilities.
Many families don't need more information. They need translation.
If you're still figuring out where to start, it can help to first find therapy and counselling resources that explain the broader mental health care system before narrowing down to a specific level of treatment.
Why families get stuck
People often assume the decision is only about symptom severity. It isn't. Daily functioning matters. Home support matters. Safety matters. Whether someone can manage time outside treatment without falling apart matters.
That's why this choice works best when you stop asking, "Which program is better?" and start asking, "What level of support fits this person's real life over a full day, not just during therapy hours?"
PHP vs IOP At a Glance
For many readers, the easiest way to understand the difference between IOP and PHP is to see the two side by side.
| Feature | PHP | IOP |
|---|---|---|
| Weekly schedule | 20 to 35 hours per week | 9 to 20 hours per week |
| Typical attendance | 5 to 7 days per week | 3 to 5 days per week |
| Daily time | 4 to 6 hours a day | 2 to 4 hours a day |
| ASAM level | Level 2.5 | Level 2.1 |
| Best fit | Higher clinical acuity, or step-down from residential | More stable daily functioning with moderate support needs |
| Daily life fit | Often feels like a full-time recovery schedule | Usually works better alongside work, school, or family life |
These time ranges come from a clinical comparison of PHP and IOP programming hours and schedule structure.
Why those hour ranges matter
Those numbers aren't just scheduling details. They reflect how much support a person needs to stay emotionally and behaviorally steady.
PHP's longer day usually means more direct observation, more structured therapeutic time, and less unstructured time during the day. IOP offers fewer treatment hours because it assumes the person can leave session, go home, go to work, or manage daily tasks without quickly losing ground.
The simplest way to think about it
If PHP and IOP were school models, PHP would be closer to a full school day with frequent staff contact. IOP would be closer to a focused class block several days a week, with much more independent time outside treatment.
That doesn't make IOP "lighter" in a dismissive sense. It just means it depends more on the person's ability to use coping skills in real settings between sessions.
Practical rule: If a person needs a lot of help staying regulated between appointments, PHP is often the closer match. If they can function between sessions and benefit from structured support that fits around life, IOP may fit better.
What families often miss in quick comparisons
A table helps, but the decision itself isn't made by hours alone. Some people look ideal for PHP on paper and still struggle because evenings at home undo the progress from the day. Others do very well in IOP because they have stable housing, supportive family, and enough emotional steadiness to practice what they learn between sessions.
That's where the deeper questions begin.
A Deep Dive into Partial Hospitalization Programs PHP
A PHP often makes sense when someone needs treatment to be the main focus of the day. The best shorthand I use with families is this: PHP is like a day job for recovery.

A person comes in for several hours, several days a week, and spends that time in a tightly organized clinical setting. The purpose isn't merely to "talk about feelings" longer. The purpose is stabilization. PHP is built for people who need more support than traditional outpatient care can provide, but who don't need overnight inpatient hospitalization.
What a PHP day often feels like
Most families imagine one long therapy appointment. It usually feels more like a structured school or workday with clinical support built into each block.
A PHP schedule may include:
- Group therapy: This is often where people practice communication, emotional regulation, coping skills, and accountability.
- Individual therapy: Some PHPs include multiple individual sessions during the week as part of the treatment structure.
- Psychiatric check-ins: Medication review and symptom monitoring may be part of care when needed.
- Skills-based work: CBT, DBT, psychoeducation, and other practical tools are often woven into the day.
A helpful local example of this level of care is a Partial Hospitalization Program near Orange County, where families can review what a full-day outpatient structure looks like in practice.
Why PHP exists
PHP corresponds to ASAM Level 2.5 and is generally used for people who need a high level of daytime structure, including those stepping down from residential care or those with symptoms that interfere with independent functioning between sessions, as described in this overview of ASAM-based PHP and IOP levels of care.
That source also notes that PHP provides daily containment for people who can't yet sustain clinical gains independently and allows real-time skill rehearsal under direct clinical supervision.
Someone in PHP isn't failing at independence. They may simply need repetition, support, and monitoring close enough together for new coping patterns to stick.
Who often benefits from PHP
PHP may be a better fit when a person is dealing with:
- Rapid symptom swings: Their mood, anxiety, cravings, or behaviors shift quickly outside structured care.
- Recent discharge from higher care: They aren't ready for a large drop in support after inpatient or residential treatment.
- Trouble holding gains between sessions: They may do well in therapy, then struggle soon after leaving.
Families sometimes worry that PHP sounds "too serious." I usually tell them that it often prevents bigger crises by adding support early, when a person is struggling but still appropriate for outpatient treatment.
A Deep Dive into Intensive Outpatient Programs IOP
If PHP is a day job for recovery, IOP is more like a strong part-time framework that helps a person practice recovery in real life while still receiving steady support.

Many people get thrown off by the word intensive. In IOP, intensive doesn't mean all day. It means the care is more involved than weekly therapy and is scheduled often enough to create momentum, accountability, and skill-building.
What IOP usually looks like
An IOP week often centers on shorter sessions held several days each week. The structure is designed so someone can attend treatment while still participating in daily responsibilities.
According to this comparison of IOP placement, structure, and therapy format, IOP is appropriate when a patient can manage daily responsibilities without decompensation. That same source explains that group therapy often makes up the core 2 to 3 hour session, while individual therapy is often added weekly.
Why some people do better in IOP than PHP
IOP works well when treatment needs to live alongside everyday life, not replace it during the day. A person may go to work, attend school, care for children, or handle household responsibilities, then come to treatment and process what happened in their daily life.
That gives IOP a different kind of value. Instead of spending most of the day in a clinical setting, the person gets repeated chances to test coping skills in normal life and bring those experiences back to the group.
A detailed example of this level of care is a mental health IOP program in Orange County, where the structure is built around therapeutic support with room for daily responsibilities.
The best fit for IOP
IOP is often a strong option for people who have enough stability to leave treatment and continue functioning until the next session. That doesn't mean they're symptom-free. It means they can stay safe and reasonably steady with support.
Here are common signs that IOP may fit:
- Stable home routine: Home isn't perfect, but it's predictable enough to support treatment.
- Ability to self-manage between sessions: The person can use coping tools, reach out, and return to session without quickly unraveling.
- Need for flexibility: Work, school, or parenting still need to continue.
IOP asks a different question than PHP. Not "Does this person need help?" but "Can this person use help well in the spaces between sessions?"
How to Decide Which Program Is Right for You
This is the point where families want a clean formula. There usually isn't one. A better decision comes from looking at the full picture of someone's day, not just the diagnosis or the schedule.
Start with daily stability
One of the biggest placement questions is simple: what happens when treatment ends for the day?
If a person leaves treatment and can eat, rest, communicate, use coping tools, avoid major triggers, and return the next day without falling apart, a lower level of structure may work. If they tend to spiral quickly once they are alone or back in their usual environment, more support may be needed.
A useful framework for these conversations is this guide on how to know which level of care in treatment is best, which helps families think through intensity, stability, and functional needs.
The home environment risk paradox
This is the part that many simple comparison articles skip. PHP can offer more treatment hours and still be less protective than people expect if home is where the biggest risk lives.
A clinical discussion of residential, PHP, and IOP differences notes that while PHP offers high intensity, returning home nightly can be a serious liability for people with strong environmental triggers. It points out that relapse often occurs during the 15+ hours a person is not in the program.
That changes the conversation.
If home includes active conflict, access to substances, unstable housing, unsafe relationships, or constant emotional activation, the question isn't only "PHP or IOP?" The question may be whether outpatient care is enough without stronger environmental support.
More hours in treatment don't automatically outweigh a harmful evening environment.
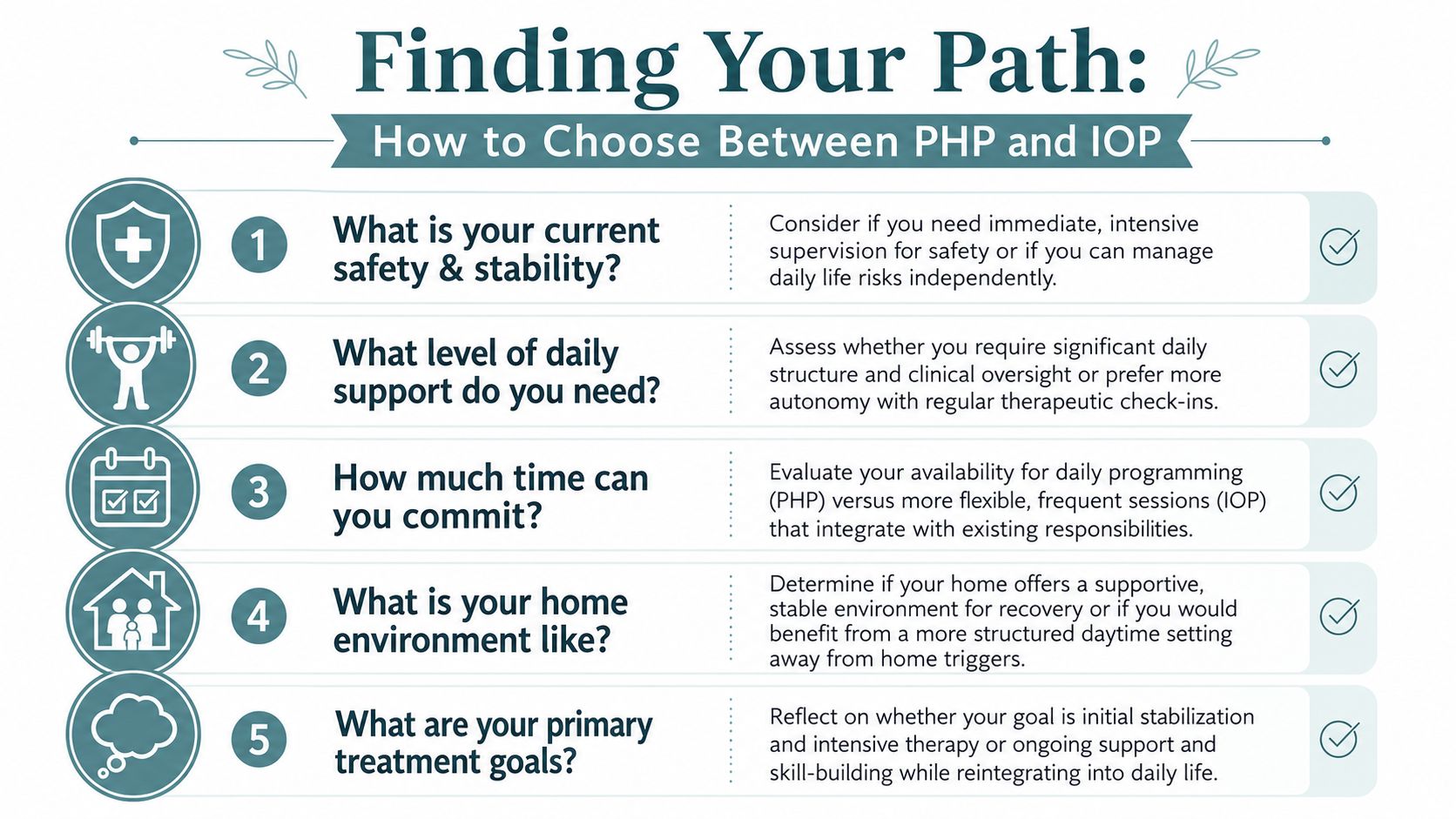
Questions worth asking before choosing
Instead of asking which label sounds stronger, ask:
- What happens after dinner: Does the person get calmer at home, or more dysregulated?
- Who is in the house: Are the people around them supportive, unpredictable, or actively triggering?
- Can they function between sessions: Can they hold onto progress for a meaningful stretch of time?
- What is the immediate goal: Is it stabilization, or is it skill practice while returning to ordinary life?
- Is step-down realistic right now: Sometimes a person needs a bridge from higher care. Sometimes they need more than a daytime bridge.
A more honest way to choose
When families understand the difference between IOP and PHP, they often stop seeing the choice as "more versus less." They start seeing it as structure versus independence, and clinical support versus environmental risk.
That shift matters. It leads to better questions, better intake conversations, and safer decisions.
Navigating Insurance Costs and Care at Casa Recovery
Money worries are often sitting underneath every treatment conversation. Families may understand the clinical recommendation and still wonder whether insurance will approve it, how long authorization may last, and why one program costs more than another.
Why PHP usually costs more than IOP
The cost difference is tied to intensity. A review of PHP versus IOP costs and ASAM coverage standards explains that PHP is generally more expensive because it involves more clinical hours, more staff time, and more facility use than IOP.
The same source notes that the American Society of Addiction Medicine, or ASAM, criteria are the foundational standard insurers use to determine coverage and clinical appropriateness for these levels of care.
That means insurance companies aren't supposed to choose a level of care based only on preference. They look at documented medical necessity. In plain language, they want to see why this person needs this amount of support right now.
What that means for families
A few practical points usually help:
- Medical necessity matters: The recommendation needs to match symptoms, functioning, and safety needs.
- Authorization can change: Coverage is often reviewed over time as the person's stability changes.
- Intensity drives cost: More hours and more clinical oversight generally mean higher program expense.
If you're comparing broader plan options before treatment, resources on 2026 Florida health insurance plans may help you understand policy structures and out-of-pocket considerations, especially if you're trying to make sense of PPO coverage.
For families considering Casa Recovery, the admissions process includes insurance verification and guidance on outpatient levels of care. That kind of support can make the financial side feel less opaque, especially when you're already juggling clinical decisions.
Frequently Asked Questions About PHP and IOP
Can someone start in PHP and later move to IOP
Yes. That pathway is common. A person may begin with a more structured daytime schedule and move into IOP once they can hold gains with more independence between sessions.
Placement isn't supposed to be a fixed identity. It should respond to how the person is functioning.
Can someone move back up from IOP to PHP
They can. If symptoms increase, functioning drops, or the person stops staying stable between sessions, a higher level of support may be appropriate.
Families sometimes see this as a setback. Clinically, it may be a better match to current needs.
The right level of care is the one that fits the person today, not the one they hoped they would still fit.
Is IOP enough if someone is still struggling
Sometimes yes, sometimes no. The key question is whether the person can manage daily responsibilities and stay reasonably stable outside treatment hours. If they can't, IOP may not provide enough structure.
Does PHP mean inpatient treatment
No. PHP is still outpatient treatment. The person attends programming during the day and returns home at night.
That return home is exactly why the home environment needs honest attention.
Are families involved in treatment
In many programs, yes. Family involvement may include therapy, education, and communication about support strategies. This can be especially helpful when home dynamics affect recovery or symptom stability.
Which is better for dual diagnosis
Neither is automatically "better." The better fit depends on the person's symptom severity, substance use pattern if present, psychiatric needs, and ability to function outside sessions. For people with co-occurring mental health and substance use concerns, integrated care matters more than the label alone.
How long do PHP and IOP last
There isn't one fixed timeline that works for everyone. Duration varies based on progress, functioning, symptom stability, and ongoing clinical review.
What should I ask on an intake call
Start with clear, practical questions:
- What level of support do you recommend and why
- How do you assess safety outside program hours
- How much individual therapy, group therapy, and psychiatric support are included
- How do families participate
- What happens if the current level of care isn't enough
If you're sorting through PHP, IOP, and what your family needs next, Casa Recovery offers information about outpatient mental health and dual-diagnosis treatment in Orange County, including PHP and IOP options, insurance verification, and admissions guidance so you can have a clearer conversation about fit.