You may be reading this because weekly therapy isn't enough, but the idea of checking into a hospital or residential program feels too big, too disruptive, or not necessary. Maybe you're getting through work meetings, answering texts, and taking care of basic responsibilities, but underneath that, things feel shaky. Your mood is harder to manage. Cravings are stronger. Anxiety, depression, trauma symptoms, or alcohol and drug use may be crowding out the life you want.
That in-between place is where many adults get stuck. They know they need more help, but they don't know what kind. An intensive outpatient program for adults is often the missing middle. It offers real clinical structure while letting you sleep at home, stay connected to your life, and practice recovery skills in your own environment.
A lot of articles describe IOP as something you do only after residential treatment. That does happen. But it misses a major truth. For many adults, IOP can also be an early, first-line level of care that helps stabilize symptoms and prevent a hospital admission when someone is struggling but can still function safely in the community.
Table of Contents
- Understanding the Levels of Care IOP vs PHP and Residential
- A Day in the Life What an Adult IOP Schedule Looks Like
- The Clinical Core of IOP Therapies and Support
- Integrated Care for Dual Diagnosis and Mental Health
- Who Is the Right Fit for an Intensive Outpatient Program
- Navigating Admissions Insurance and Your First Steps
- Frequently Asked Questions About Adult IOP
Understanding the Levels of Care IOP vs PHP and Residential
Mental health and addiction treatment are organized into levels of care based on how much structure, monitoring, and support a person needs right now.
That matters because many adults wait too long to get help. They keep trying to manage with weekly therapy alone, even when symptoms are getting harder to contain at home or work. In many cases, an intensive outpatient program can serve as an early, first-line option that adds enough support to prevent a crisis from turning into an emergency room visit or hospitalization.
The goal is to match the treatment setting to the current level of risk and impairment. Too little support can leave someone stuck. Too much restriction can disrupt work, parenting, and daily life when a less intensive setting could still work well.
Practical rule: Choose the lowest level of care that provides enough structure for safety, symptom relief, and steady progress.
For many adults, IOP fits that middle space. It offers repeated contact with a clinical team, regular therapy, and accountability during the week, while you continue living at home and practicing new skills in real situations.
Comparing levels of care side by side
Here is the clearest way to separate the three common options.
| Feature | Residential Treatment | Partial Hospitalization (PHP) | Intensive Outpatient (IOP) |
|---|---|---|---|
| Housing | You live at the facility | You live at home or in supportive housing | You live at home or in supportive housing |
| Daily structure | Full-day and overnight support | Most of the day in treatment | Several therapy blocks across the week |
| Clinical focus | Safety, stabilization, and a fully contained setting | High daytime support with close monitoring | Frequent therapy and skill practice while living in the community |
| Best fit | Adults who need 24-hour supervision or a major break from their environment | Adults who need more support than IOP but do not need overnight care | Adults who need more than weekly therapy and can remain safe outside a hospital |
A simple way to read this table is to ask one question: how much support do I need between sessions?
Residential treatment places support around the entire day and night. PHP concentrates treatment into most of the day, several days a week. IOP works more like a strong brace than a full cast. It adds meaningful support and structure, but it still lets you walk through daily life and notice where you need more practice.
If you are weighing these two outpatient options, this guide on how IOP differs from PHP explains the day-to-day distinction in plain language.
IOP also should not be viewed only as the place people go after residential care. For many adults, it is the first serious level of treatment that matches the problem. Someone may be struggling with panic, depression, relapse risk, mood instability, or dual diagnosis symptoms that are too intense for weekly outpatient care, but not severe enough to require 24-hour supervision. In that situation, IOP can provide early, intensive support before the situation worsens.
Research on substance use treatment has found that intensive outpatient care can produce outcomes comparable to inpatient treatment for many people. The practical takeaway is straightforward. A person does not always need the most restrictive setting to make meaningful progress. They need a setting with enough repetition, clinical contact, and structure to interrupt the current pattern.
A Day in the Life What an Adult IOP Schedule Looks Like
You wake up knowing something has to change, but a hospital stay feels too disruptive and one therapy appointment a week has not been enough. This is the space IOP is designed to fill. It gives adults a concentrated block of treatment each week while they continue living at home, going to work, caring for family, and practicing new skills in real life.
Most programs are built around a weekly treatment schedule, not an all-day, every-day format. Medicare describes IOP as appropriate for people who need at least 9 hours per week of therapeutic services in an outpatient setting through its intensive outpatient program coverage guidance. In practice, that usually means three to five days of treatment each week, often in half-day blocks.
What the weekly commitment usually feels like
A good way to picture the rhythm is physical therapy after an injury. A single appointment can point you in the right direction. Repeated sessions each week are what help you build strength, catch setbacks early, and replace habits that keep reopening the same problem.
That repetition matters. For an adult dealing with panic, depression, substance use, trauma symptoms, or mood instability, the goal is not only to talk about what is wrong. The goal is to create enough contact and structure each week that treatment starts affecting Tuesday afternoon, not just the hour you are in session.
This is one reason IOP can serve as an early, first-line intervention, not only a step after higher levels of care. If symptoms are intensifying and weekly outpatient therapy is no longer containing the problem, IOP can add support before a crisis leads to the emergency room or hospitalization.
A sample rhythm for the week
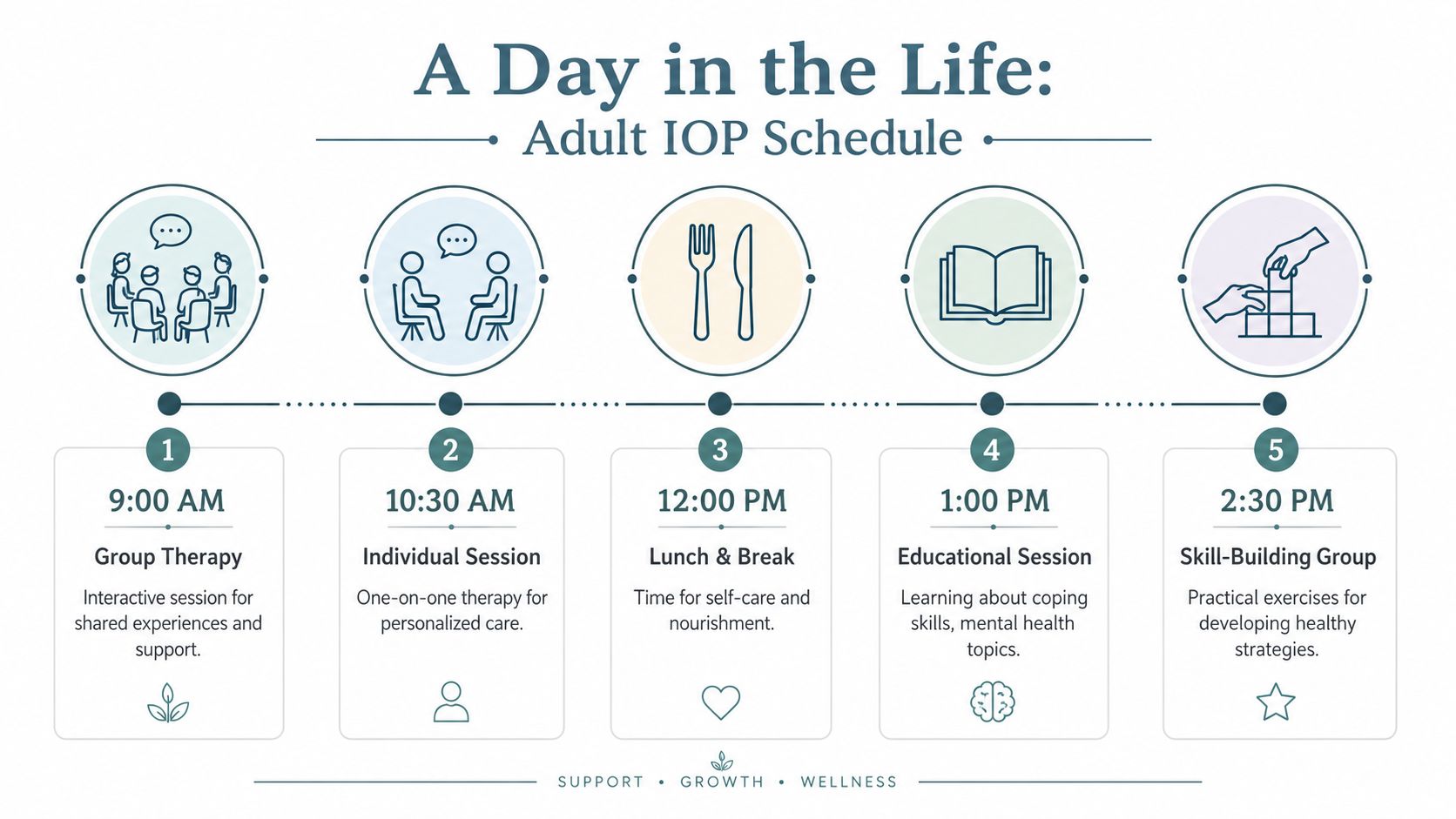
No two programs use the exact same calendar, but many adult IOP schedules include a mix like this:
- Group therapy blocks: Several sessions each week focused on coping skills, emotional regulation, relapse prevention, or symptom management.
- Individual therapy: One-on-one sessions to work through personal history, treatment goals, barriers, and progress.
- Educational sessions: Practical teaching on subjects like triggers, trauma responses, communication, boundaries, sleep, and recovery planning.
- Psychiatric support: Medication evaluation and follow-up when needed.
- Family involvement: Some programs offer family sessions or education so home support becomes clearer and more consistent.
On paper, that can still feel abstract.
Reviewing a sample weekly IOP schedule for adults often makes the time commitment easier to judge. You can see how treatment blocks fit into a normal week and whether the structure feels realistic for your life.
A well-designed IOP schedule should create momentum without making attendance impossible. You should feel stretched, supported, and able to keep showing up.
The Clinical Core of IOP Therapies and Support
An intensive outpatient program for adults isn't just extra therapy appointments. Its value stems from how different pieces of care work together.
Why group therapy matters so much
Many adults hear "group therapy" and assume it means sitting in a circle and listening to strangers talk. Good group therapy is much more active than that.
Groups give you a place to test out honesty, boundaries, emotional regulation, and communication in real time. If depression tells you to isolate, or addiction tells you no one understands, a well-run group directly challenges that story. You hear your own patterns reflected back by people who recognize them.
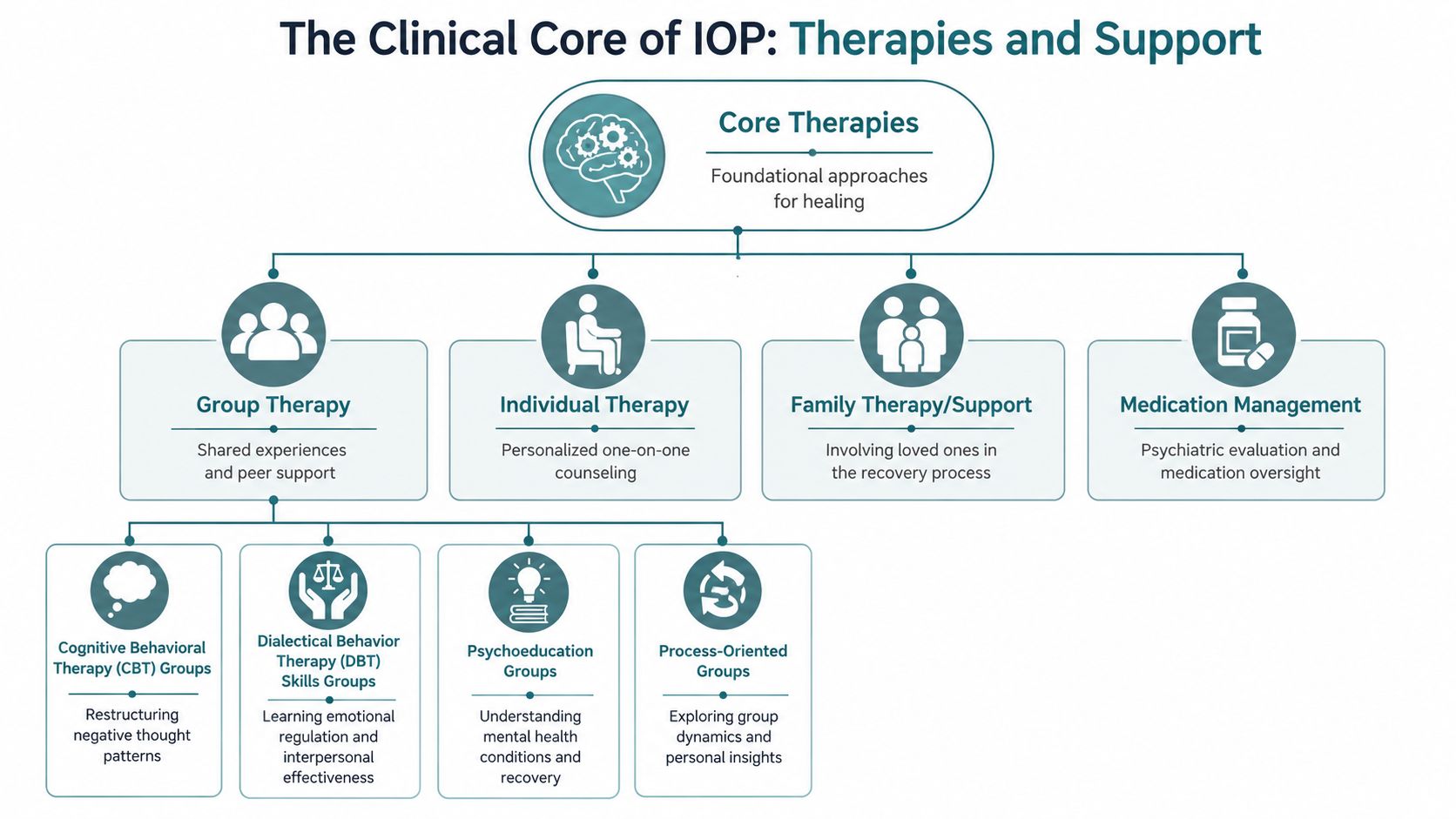
Common group formats in IOP include:
- CBT groups: These focus on the link between thoughts, feelings, and behaviors. You learn how to identify distorted thinking and replace it with more useful responses.
- DBT skills groups: These teach emotional regulation, distress tolerance, mindfulness, and interpersonal effectiveness.
- Psychoeducation groups: These help you understand what symptoms mean, how triggers work, and what relapse or destabilization tends to look like before it fully happens.
- Process groups: These are less about worksheets and more about what happens between people in the room, which often mirrors what happens outside treatment.
What individual therapy and psychiatry add
Group work is powerful, but it doesn't replace private clinical work.
In individual therapy, you can talk about the parts of your story that don't belong in a group setting yet. That may include trauma, grief, family conflict, shame, self-harm urges, or the details of substance use. The therapist can also tailor treatment goals to your life. Not a generic recovery plan, but your recovery plan.
Psychiatric care matters too. Adults entering IOP may be dealing with sleep disruption, panic, mood swings, depression, trauma symptoms, or medication questions. Onsite psychiatric evaluation and medication management can help align the medical side of care with the therapy side, instead of treating them like separate worlds.
One outpatient option in Orange County is Casa Recovery, which offers adult PHP and IOP, integrated dual-diagnosis treatment, onsite psychiatry, family programming, and evidence-based modalities including CBT, DBT, EMDR, Brainspotting, Motivational Interviewing, art therapy, and denial management.
Evidence-based therapies you may see in IOP
Not every person in IOP needs the same methods. The strongest programs match therapies to the problem in front of them.
For example:
- CBT helps when your thinking keeps spiraling toward hopelessness, fear, or all-or-nothing reactions.
- DBT helps when emotions rise fast and decisions happen even faster.
- Motivational Interviewing helps when part of you wants change and another part isn't ready.
- EMDR and other trauma therapies can help when trauma symptoms are feeding anxiety, dissociation, or substance use.
Trauma treatment in outpatient care often surprises people. They assume trauma work only belongs in long-term residential settings. But trauma-focused IOP models using EMDR and Prolonged Exposure have shown a 65% PTSD diagnosis remission rate within six treatment days and a 4% dropout rate in the evidence summarized by Epic Health Partners on evidence-based outpatient treatment.
That doesn't mean every person should start trauma processing immediately. It means outpatient care can be clinically deep, not just supportive.
Integrated Care for Dual Diagnosis and Mental Health
Many adults who seek IOP are not dealing with a single issue in isolation. They may be drinking every night to calm panic symptoms, using pills to sleep through trauma-related nightmares, or cycling between depression and substance use in a way that is hard to untangle on their own.
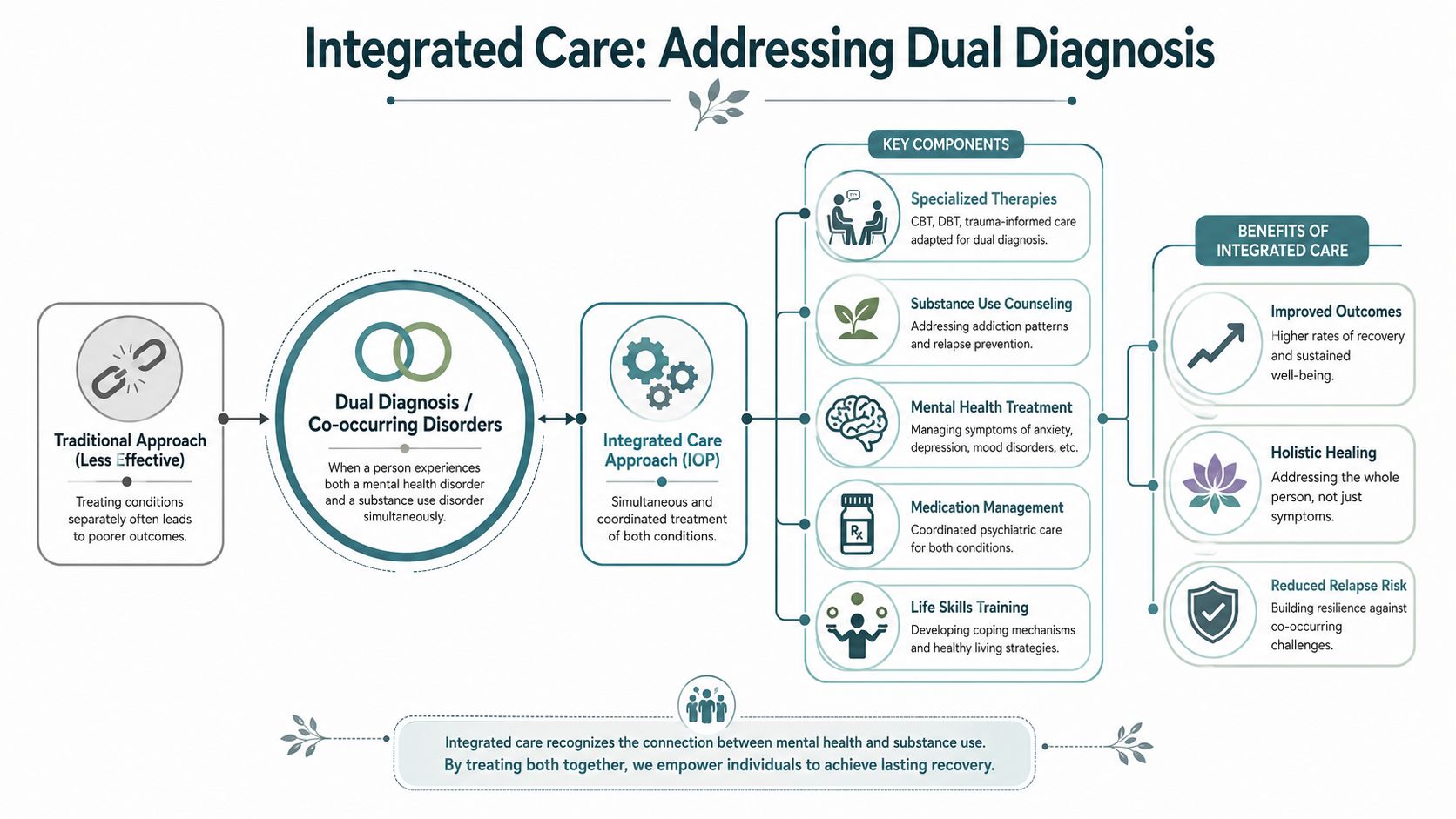
That pattern has a name. Dual diagnosis, also called co-occurring disorders, means a person has both a mental health condition and a substance use disorder at the same time.
What dual diagnosis actually means
Dual diagnosis does not mean someone has "two separate problems" that can be treated on separate tracks. In real life, the conditions usually interact. Anxiety can increase alcohol use. Alcohol can worsen depression. Trauma can make both treatment attendance and emotional regulation harder.
That is why integrated care matters in IOP, especially when the goal is to stabilize someone early and keep symptoms from building into a crisis that requires hospitalization. Instead of waiting until life fully falls apart, an adult can enter IOP as a first-line intervention and get several forms of support at once. Therapy addresses the emotional drivers. Recovery work addresses substance use patterns. Psychiatry, when needed, helps with medication evaluation and symptom monitoring. Skills practice helps the person function at home, at work, and in relationships.
As noted earlier, co-occurring mental health needs are common in adult outpatient treatment. Programs that treat only one side of the picture often miss the pattern that keeps the cycle going.
Why integrated treatment works better
Fragmented care puts too much burden on the patient. One clinician may focus on drinking or drug use. Another may focus on panic, mood, or trauma symptoms. The adult in treatment becomes the person trying to connect everything, explain everything twice, and figure out which problem to tackle first.
Integrated IOP is built to handle the full pattern in one setting. If cravings rise after a trauma trigger, the team can respond to both. If depression makes it hard to attend groups, that is treated as part of the care plan, not as a separate failure. A good program looks for the links between symptoms, behavior, and environment in the same way a good primary care doctor looks at the whole body, not just one lab result.
For families who want a clearer understanding of how emergencies are identified and handled, ProMed Certifications offers a useful overview of mental health crisis intervention in plain language.
If you want a closer look at why concurrent care matters, this guide on understanding dual diagnosis and treating both mental health and addiction together explains how integrated treatment supports longer-term stability.
Treating co-occurring disorders together often makes the difference between brief relief and real progress that holds up outside the therapy room.
Who Is the Right Fit for an Intensive Outpatient Program
A common adult IOP referral sounds like this: someone is still showing up to work, still answering texts, still paying rent, but life is taking more effort every week. Sleep is getting worse. Anxiety is louder. Drinking or drug use is creeping up. Weekly therapy no longer holds things steady, yet hospitalization still feels one step too far.
That middle zone is often where IOP fits best.

IOP works for adults who need more structure, more contact, and more skill practice than standard outpatient care provides, while still being able to live at home and take part in daily life. A simple way to understand it is to compare it to medical care. Weekly therapy can feel like a regular office visit. Residential treatment is closer to staying in the hospital. IOP sits in between. It gives repeated care during the week so problems can be addressed early, before they become emergencies.
Adults who often do well in IOP
Adults are often a good match for IOP when several of these are true:
- Weekly therapy is not enough anymore: You may be trying hard, but symptoms keep flaring between sessions. More frequent treatment gives you more chances to practice skills while real life is still happening.
- You want to prevent a higher level of care: IOP is often used after residential treatment or PHP, but that is only part of the picture. It can also be the first serious intervention when things are sliding and you want to stop that slide early.
- Home is stable enough for recovery work: You do not need a perfect environment. You do need a place where you can sleep, return after treatment, and stay reasonably safe.
- You can attend consistently: Motivation can rise and fall. What matters is enough ability and willingness to show up, participate, and keep working even on hard days.
- Your symptoms are significant, but you do not need 24-hour supervision: Many adults in IOP are struggling in a very real way, yet can still use a safety plan, reach out for help, and remain in the community.
Many adults hesitate because they believe IOP is only for people who have already "failed" weekly therapy or already completed residential care. Good placement does not work that way. Clinicians look at current symptoms, safety, functioning, and how much support is needed now.
Signs IOP may be the right level now
A person may be a strong candidate for IOP if daily life is narrowing. Maybe getting out of bed takes much more effort. Maybe panic is making it hard to drive, shop, or focus. Maybe alcohol or drugs have become the main coping tool after daily demands. Maybe there have been recent emergency room visits, intense mood swings, or growing isolation, but the person can still participate in treatment and does not need overnight monitoring.
IOP is not just a step-down service; it is often a first-line option for adults who need intensive help quickly to avoid a deeper crisis. In plain terms, it can be the treatment that catches someone before hospitalization becomes necessary.
A helpful question is not, "Am I sick enough?" The better question is, "Do I need more support than one appointment a week can give?"
When IOP may not be enough
IOP is not the best fit for every situation. Adults who cannot stay safe outside of a supervised setting, are at imminent risk of harming themselves or others, are experiencing severe medical or psychiatric instability, or cannot reliably return to a safe living environment may need PHP, inpatient care, residential treatment, or emergency services instead.
That distinction protects people. The goal is not to choose the least intensive option. The goal is to choose the level of care that matches the actual level of risk and support needed.
Practical factors also matter. If transportation, hearing, vision, language access, or digital access could affect participation, ask direct questions before enrolling. These issues can shape whether treatment is usable in real life, and broader discussions about accessibility in healthcare can help families know what to ask for.
A good IOP fit usually means this: symptoms are serious, life is getting harder to manage, and more frequent treatment could stabilize things before they become unsafe.
Navigating Admissions Insurance and Your First Steps
Starting treatment often feels hardest before the first call. People worry they'll say the wrong thing, find out insurance won't help, or get pushed into a program that doesn't fit.
The process is usually much simpler than people expect.
What usually happens first
Most admissions pathways begin with a confidential conversation. You describe what has been happening, what symptoms or substance use concerns are showing up, whether you're safe, and what kind of help you're looking for. From there, the program can discuss scheduling, verify benefits, and decide whether an assessment is the next step.
A basic flow often looks like this:
- Phone consultation: You share your concerns and ask questions.
- Insurance verification: The provider checks behavioral health benefits and coverage details.
- Clinical assessment: A clinician evaluates symptoms, history, risks, and level-of-care needs.
- Scheduling and orientation: If IOP fits, the team helps you plan a start date.
What to ask before you enroll
It's okay to be direct. Ask whether the program treats your specific issues, whether psychiatry is available, how family involvement works, and what the weekly schedule looks like.
If digital access matters to you or a family member, it can also help to understand broader issues around accessibility in healthcare, especially when forms, portals, and communication tools are part of the intake experience.
For readers evaluating local options, Casa Recovery states that it accepts PPO plans from all carriers and is in network with Blue Shield of California/Blue Card, ComPsych, and Holman Group, while also providing insurance verification and admissions guidance. The most useful next step is usually a direct benefits check and a clinical conversation about fit.
Frequently Asked Questions About Adult IOP
A common question sounds like this: "I am struggling, but I am still getting up, going to work, answering emails, and taking care of people. Do I really need something as intensive as IOP?" For many adults, that is exactly where IOP fits. It offers more support than weekly therapy while letting you stay connected to daily life, which is often the setting where stress, triggers, and recovery skills show up in real time.
Can I work or go to school during IOP
Often, yes.
IOP is built for adults who need several hours of treatment each week but do not need 24-hour supervision. Many programs offer morning, evening, or virtual options, so work, school, parenting, or caregiving can continue with some planning. The question is less about whether your calendar is full and more about whether your current responsibilities leave enough room to participate, practice new skills, and rest.
A good rule of thumb is to picture IOP as adding a part-time job focused on your health. If your life can make room for that commitment, IOP may be workable.
How is family involved
Family involvement depends on the program and on what you want. For some adults, a spouse, parent, or other support person joins family sessions or educational meetings. For others, treatment stays more private.
When family participation is a fit, it can help in very practical ways. Loved ones may learn how symptoms affect behavior, how to respond during a hard week, and how to support progress without slipping into arguing, rescuing, or constant monitoring. That often lowers tension at home and gives everyone a clearer role.
What happens after IOP ends
IOP is usually one phase of care, not the whole plan. After discharge, many adults continue with individual therapy, medication management, peer support, family work, or a lower level of outpatient treatment.
That gradual step-down matters. It works like taking the training wheels off over time instead of all at once. The goal is not to keep you in treatment forever. The goal is to help you carry the gains of treatment into ordinary life with enough support still in place.
Is IOP effective enough if I do not go inpatient
For many adults, yes. Earlier in this article, we noted research showing that intensive outpatient treatment can produce outcomes similar to inpatient care for many people with substance use disorders.
That matters because IOP is not only a step after residential treatment. It can also serve as an early, first-line intervention for adults who need more than weekly therapy and want to avoid a crisis getting worse. If you are stable enough to remain safe at home, a well-matched IOP can provide frequent clinical contact, structure, and accountability before hospitalization becomes necessary.
How do I know if I need IOP or something more intensive
A clinical assessment is the safest way to answer that. Symptoms can look manageable from the outside while becoming hard to control behind the scenes. A trained clinician looks at safety, substance use, mental health symptoms, medical needs, daily functioning, and your support system.
In simple terms, the decision often comes down to this: Can you stay safe and use treatment while living in the community? If yes, IOP may fit. If you are medically unstable, at immediate risk, or unable to function without close supervision, a higher level of care may be needed.
If you're trying to decide whether outpatient care is enough, you do not have to figure it out alone. Casa Recovery offers adult outpatient mental health and dual-diagnosis treatment in Orange County, including IOP and PHP. A confidential consultation can help you understand your options, verify insurance, and decide what level of support fits your situation right now.