You may be living in a pattern that feels impossible to name. Your son says he drinks because his anxiety is unbearable. Your partner stops using for a few days, then the depression crashes in and the pills come back. You try to focus on one problem at a time, but every attempt seems to wake up the other one.
That confusion has a clinical name. It's called co-occurring disorders, also known as dual diagnosis. It means a person is dealing with a mental health condition and a substance use disorder at the same time. Once families hear that term, many feel two things at once: relief that this has a name, and fear that it sounds more complicated than they expected.
Both reactions make sense. The good news is that this pattern is understood, it's treatable, and there's a clear path forward when care is designed to address the whole picture instead of just one piece.
Table of Contents
- The Invisible Struggle of a Dual Diagnosis
- What Are Co-Occurring Disorders and How Do They Interact
- Recognizing the Signs of a Dual Diagnosis
- Why Integrated Treatment Is the Only Path Forward
- What Integrated Dual Diagnosis Treatment Involves
- Family Involvement and Navigating the First Steps to Care
- Taking the Next Step in Orange County
The Invisible Struggle of a Dual Diagnosis
A dual diagnosis often hides in plain sight. A family may see panic attacks and assume the drinking is secondary. Or they may focus on marijuana, alcohol, opioids, or stimulants and miss the severe mood swings, trauma reactions, or hopelessness underneath. Everyone is reacting to what hurts most in the moment.
A common family story sounds like this: “When she stops drinking, her anxiety gets worse. When her anxiety gets worse, she drinks again.” That isn't stubbornness or lack of willpower. It's often a sign that two conditions are locked together, each making the other harder to treat.
Why this feels so hard to untangle
Mental health symptoms and substance use don't line up neatly. They overlap. Irritability can come from withdrawal, depression, trauma, sleep disruption, or all four. Isolation can look like shame, intoxication, exhaustion, or fear. Families often blame themselves because nothing they try seems to work for long.
Practical rule: If a person keeps getting worse when only one side of the problem is treated, assume both need attention.
This is also far more common than many people realize. Approximately 21.5 million adults in the United States experienced both a mental illness and a substance use disorder in the past year. Despite this, 41.2% received no treatment at all, leaving nearly 8.8 million people without adequate support according to this overview of co-occurring disorders and treatment gaps.
You are not dealing with something rare
When families finally hear “dual diagnosis,” they often say, “I thought it was just us.” It isn't. This pattern shows up in homes that look stable from the outside, in young adults who seem high functioning, and in people who've tried treatment before but never got a full explanation of what was happening.
Naming the problem doesn't solve it by itself. But it does stop the guessing. And that's where recovery starts.
What Are Co-Occurring Disorders and How Do They Interact
The simplest definition is this: co-occurring disorders means a person has at least one mental health disorder and at least one substance use disorder at the same time. The important part isn't just that both exist. It's that they interact.
Families often ask, “Which came first?” That's a fair question, but it can become a trap. Clinically, this is often a chicken-and-egg problem. Sometimes anxiety, depression, trauma, bipolar symptoms, or another condition shows up first, and the person starts using substances to quiet the distress. Sometimes heavy substance use changes mood, sleep, energy, thinking, and behavior so much that mental health symptoms emerge or get sharply worse.
Why the two conditions feed each other
Imagine a house with both a roof leak and damaged wiring. If you only patch the ceiling stain, the leak continues. If you only fix one wire but ignore the water, the electrical problems return. Co occurring disorders and addiction work in a similar loop.
A person might drink to slow racing thoughts. At first, that may feel like relief. Later, alcohol can increase depression, worsen sleep, lower frustration tolerance, and create withdrawal symptoms that feel like intense anxiety. The person then drinks again to escape the very symptoms the substance is helping create.
That feedback loop is why single-issue treatment often falls short. If you want a helpful plain-language companion on this topic, this guide on navigating co-occurring conditions gives families another way to understand the overlap.
Common co-occurring disorder pairings
The pairings below aren't diagnoses by themselves. They're examples of patterns clinicians often assess when symptoms and substance use are tightly linked.
| Mental Health Condition | Commonly Paired Substance | Typical Interaction |
|---|---|---|
| Anxiety | Alcohol | A person may drink to feel calmer in social situations or at night, then rebound anxiety can intensify after use wears off. |
| Depression | Alcohol or opioids | Substances may briefly numb sadness or emptiness, but often deepen low mood, isolation, and loss of motivation. |
| Trauma-related symptoms | Opioids, alcohol, or sedatives | A person may try to shut down intrusive memories, body tension, or emotional flooding through sedation. |
| Bipolar symptoms | Alcohol, stimulants, or multiple substances | Impulsivity, poor sleep, and mood swings can increase substance use, while substances can destabilize mood further. |
| Psychotic symptoms | Cannabis, stimulants, or alcohol | Some substances can worsen confusion, paranoia, or disorganization and make treatment harder to follow. |
Treat the pair, not just the loudest symptom.
One more point often surprises families. These conditions don't always look dramatic. Some people keep a job, show up to family events, and still live in a constant private cycle of panic, shame, cravings, and emotional collapse. The outside picture can be misleading.
Recognizing the Signs of a Dual Diagnosis
Most families don't spot a dual diagnosis all at once. They notice fragments. Missed work. Sudden anger. Sleeping all day. A burst of motivation followed by a crash. A bottle hidden in the garage. A prescription used too fast. Silence where there used to be connection.
What families usually notice first
The signs often fall into a few categories.
- Behavior changes: Pulling away from friends, avoiding responsibilities, secrecy, disappearing for long stretches, or losing interest in routines that used to matter.
- Emotional swings: Irritability, panic, numbness, hopelessness, sudden tearfulness, or intense reactions that seem bigger than the situation.
- Thinking changes: Poor concentration, suspiciousness, indecision, confused explanations, or strong denial about obvious consequences.
- Physical clues: Major sleep changes, appetite shifts, low energy, agitation, shakiness, or looking unusually slowed down.
A person doesn't need every sign. What matters is the pattern. If the symptoms seem to move together, especially in cycles, that's important.
Why people miss the pattern
One reason dual diagnosis gets overlooked is that substance effects can mimic mental health symptoms. Intoxication can look like mood instability. Withdrawal can look like anxiety or agitation. Chronic substance use can flatten motivation and give the impression of severe depression.
The reverse also happens. A person with untreated trauma or panic may use substances in ways that relatives dismiss as “partying” or “stress relief,” when the behavior is an attempt to self-manage severe internal distress.
Another problem is diagnostic overshadowing. That means one issue becomes so obvious that everyone stops looking further. If the drinking is visible, people blame everything on alcohol. If the anxiety is dramatic, they may minimize the substance use. The actual clinical picture gets split in half.
If symptoms keep changing but never fully resolve, don't assume the person is being dishonest. Assume the assessment may be incomplete.
Families also get confused by timing. “He's only anxious after he uses” or “She only drinks when she's depressed” can sound like separate problems. In practice, those kinds of statements often describe a loop, not a separation.
The goal isn't for families to diagnose a loved one at home. It's to notice when the story doesn't fit a simple explanation. That's usually the moment a more complete evaluation becomes necessary.
Why Integrated Treatment Is the Only Path Forward
The old model treated addiction first and mental health later, or the other way around. On paper, that may sound organized. In real life, it often fails because the conditions are connected.
Trying to separate them is like sending your car to one shop to fix the brakes but telling that mechanic to ignore the fluid leak because another shop will handle it next month. The systems affect each other. If the work isn't coordinated, the original problem keeps returning in a new form.
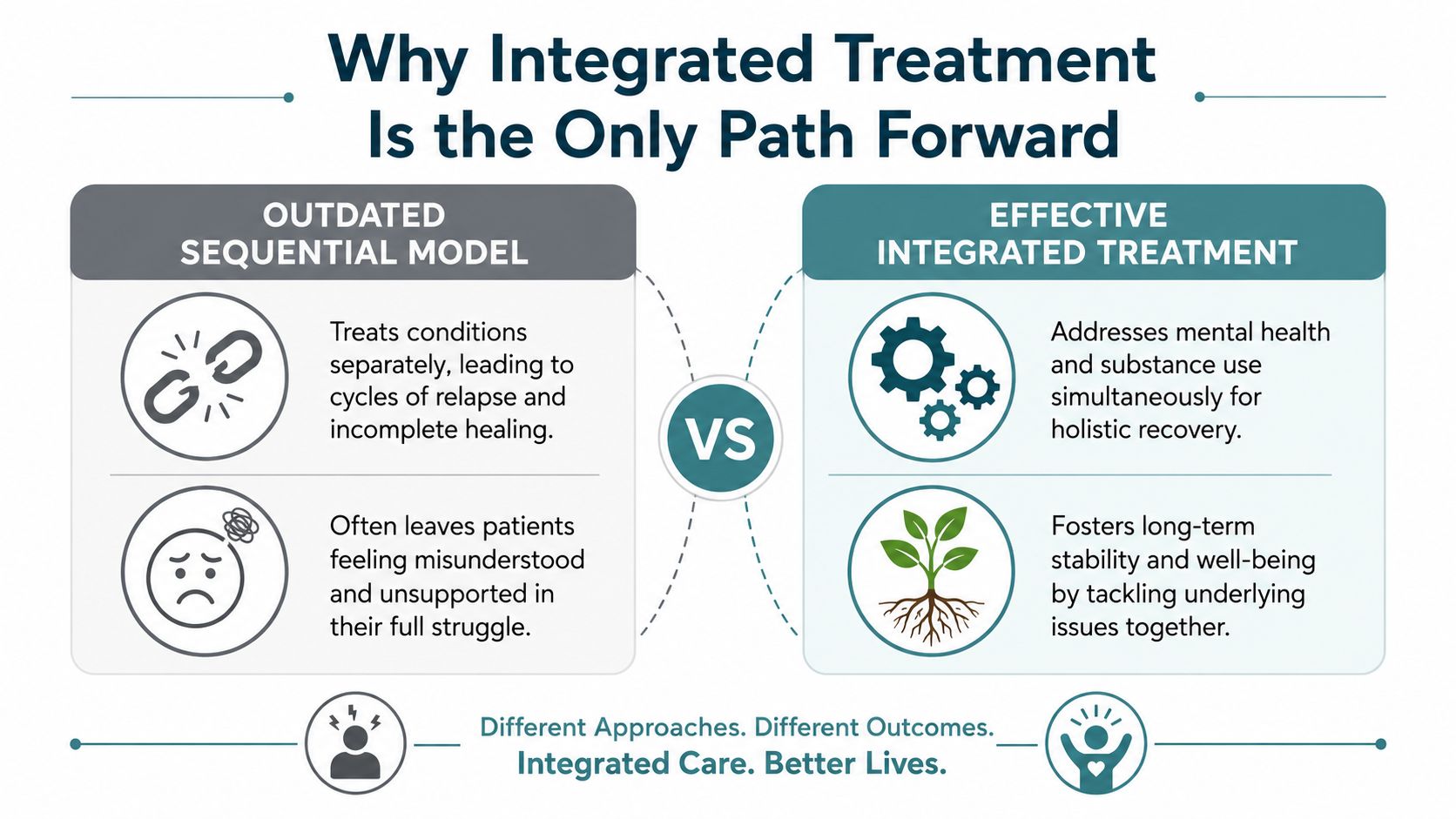
Why separate treatment often fails
In sequential care, a program may say, “Get sober first, then we'll address the trauma.” Another provider may say, “Stabilize the depression first, then we'll talk about the cocaine or alcohol.” The person ends up bouncing between doors, never treated as a whole person.
That approach can leave a patient feeling blamed from both sides. Addiction treatment may interpret psychiatric distress as resistance. Mental health treatment may underestimate how strongly cravings, withdrawal, and substance rituals drive behavior.
What integrated care does differently
Integrated care means one coordinated treatment plan addresses both conditions at the same time. The therapy goals, psychiatric evaluation, medication decisions, relapse prevention work, and family communication all line up around the same clinical picture.
The reason this matters isn't philosophical. It's practical. Individuals with co-occurring disorders face significantly worse outcomes when care is not integrated. Evidence-based integrated psychological interventions are the only modalities with solid scientific backing for reducing substance use in patients with severe mental illnesses, while pharmacological evidence for this specific comorbidity remains limited, as explained in this review of treatment outcomes for co-occurring disorders.
A strong program also avoids the trap of fragmented messaging. The therapist isn't working in one direction while psychiatry works in another. The structure supports the same goal from multiple angles. Families who want a concrete example of what that looks like can review an integrated treatment approach for co-occurring disorders.
Integrated treatment doesn't ask a person to choose which part of their suffering deserves help first.
That's why this model is the standard families should look for. Not because it sounds modern, but because it matches how the disorder works.
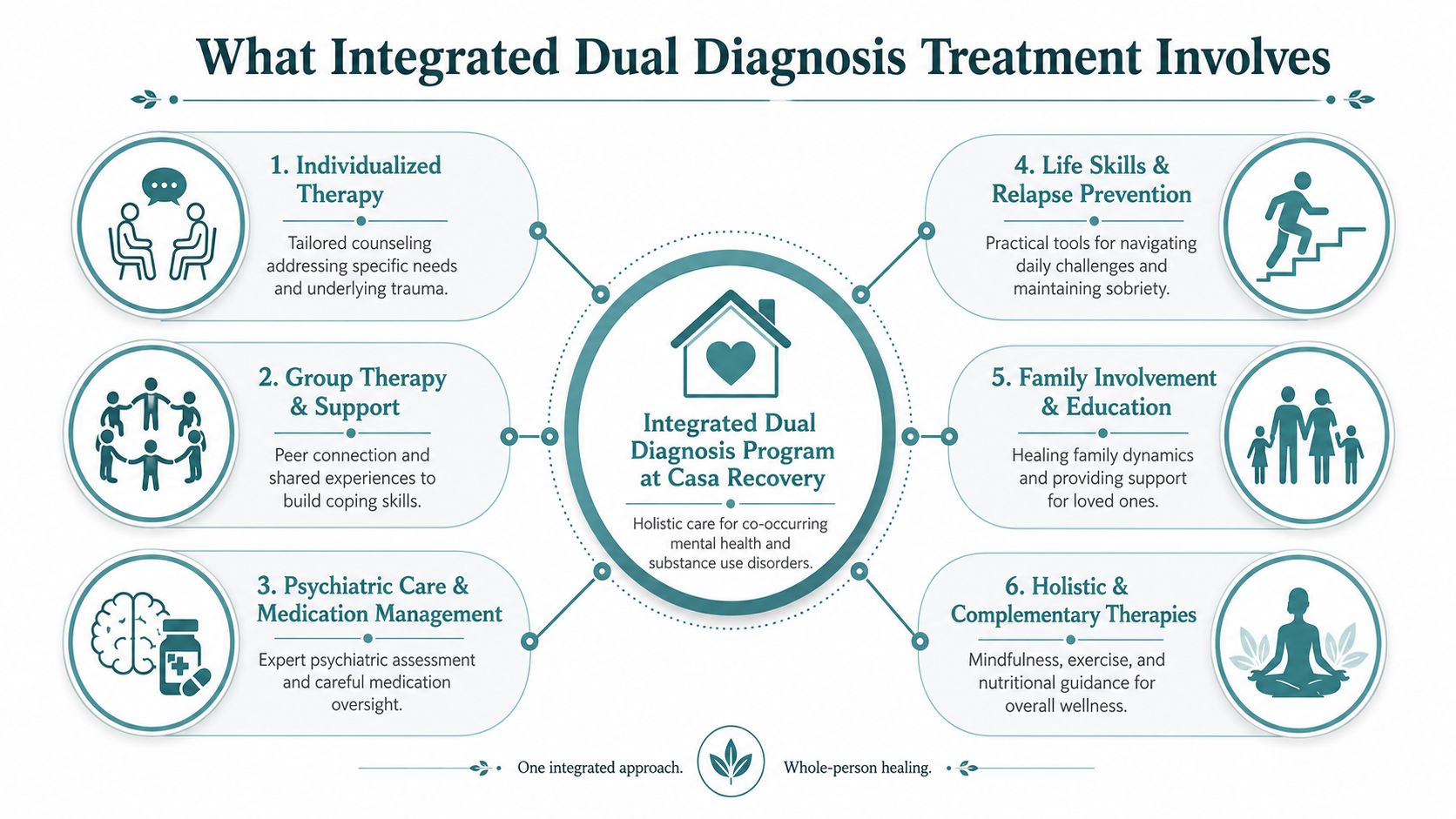
What Integrated Dual Diagnosis Treatment Involves
Once families understand why integrated care matters, the next question is usually, “What does that look like day to day?” A good dual diagnosis program is structured, layered, and flexible. It doesn't rely on one therapy session a week and hope for the best.
One reason that level of structure matters is prevalence within treatment settings themselves. Among adolescents in community-based substance use disorder treatment programs, over 60% meet diagnostic criteria for another mental illness, and in outpatient clinics, 50% of admissions have co-occurring disorders, according to this NCBI overview of co-occurring disorder prevalence and treatment systems. Dual diagnosis is often the clinical norm, not the exception.
The structure of care
Most outpatient dual diagnosis programs organize treatment by level of support.
- Partial Hospitalization Program (PHP): This is full-day structured clinical care without overnight stay. It can help people who need substantial support, close monitoring, and a strong daily routine.
- Intensive Outpatient Program (IOP): This level offers multiple treatment sessions each week while allowing more room for work, home responsibilities, or step-down recovery planning.
- Mental health track within dual diagnosis care: Some people need a plan that emphasizes depression, anxiety, trauma, or bipolar symptoms while still addressing substance use in every part of treatment.
The level of care should match the person's stability, risk, daily functioning, and support at home. More isn't always better. Better matched is better.
The clinical pieces working together
A strong integrated program combines several forms of care because each one solves a different problem.
- Psychiatric evaluation and medication management help clarify diagnosis, assess safety, and support symptom stabilization. This is especially important when sleep, mood, panic, or thought patterns are disrupting daily life.
- Individual psychotherapy gives the person room to work on their own history, triggers, beliefs, and behavior patterns. Some programs, including Casa Recovery, provide outpatient dual diagnosis care with PHP and IOP options, onsite psychiatric services, trauma-informed treatment, and frequent one-on-one therapy sessions as part of a coordinated plan.
- Group therapy and psychoeducation reduce shame and help people learn how symptoms, cravings, relationships, and relapse patterns connect.
- CBT and DBT build concrete skills. CBT helps challenge distorted thinking and harmful behavior loops. DBT helps with emotion regulation, distress tolerance, and interpersonal stability.
- Trauma therapies such as EMDR and Brainspotting matter when unresolved trauma keeps driving panic, avoidance, numbness, or self-medication.
- Motivational interviewing and relapse prevention help a person strengthen commitment, prepare for ambivalence, and create a plan for high-risk situations.
- Integrated well-being practices such as mindfulness, art therapy, exercise, and nutrition can support nervous system regulation and daily functioning.
A well-built plan should feel coordinated, not crowded. The person isn't being sent in ten directions. The services are meant to reinforce each other.
Family Involvement and Navigating the First Steps to Care
Families often carry a heavy mix of love, exhaustion, anger, and guilt. They've tried helping, confronting, stepping back, and rescuing. By the time treatment becomes a serious option, many relatives are worn down and unsure how to be useful without making things worse.
Why family participation matters
Recovery happens faster when the home environment becomes more informed and less reactive. That doesn't mean families cause the disorder. It means they can learn how not to get pulled into its patterns.
Family work often focuses on communication, boundaries, education about symptoms, and the difference between support and enabling. When a program includes formal family services, relatives get a place to ask hard questions and stop operating from panic. This overview of the importance of family involvement in treatment shows what that support can look like in practice.
Families don't need to become therapists. They do need a shared language and a calmer plan.
Some of the most helpful shifts are simple. Stop arguing with symptoms. Respond to behavior consistently. Don't mistake temporary calm for lasting stability. Learn what relapse warning signs look like before a crisis happens.
What the first call usually covers
The admissions process feels intimidating until someone explains it plainly. In most cases, the first call is a confidential conversation about what's been happening, what substances are involved, what mental health symptoms are showing up, and how urgent the situation feels.
A practical intake process often includes:
- Insurance review: Many programs can verify PPO benefits and explain whether plans are in network. Some centers also work with carriers and employer-based behavioral health partners in specific ways.
- Clinical screening: Staff usually ask about safety concerns, recent use, psychiatric history, medications, and prior treatment.
- Level-of-care discussion: The team helps determine whether PHP, IOP, or another setting fits the person's needs.
- Logistics planning: If the client lives outside the immediate area, supportive living options and scheduling details may also be discussed.
The purpose of that call isn't pressure. It's clarity.
Taking the Next Step in Orange County
If you're in Orange County, you don't need to solve this alone before reaching out. The next step can be small. A phone call. An insurance check. A quiet conversation where you describe what you've been seeing and ask whether it sounds like a dual diagnosis.
Some families want to compare options first, and that's reasonable. If you're looking for broader context on specialized dual diagnosis care in Orange County, that resource can help you understand what local programs may offer and what questions to ask.
For residents in South Orange County, support for co-occurring disorders in San Juan Capistrano and nearby communities can make the search feel more concrete. Local access matters when families are trying to coordinate work, transportation, therapy schedules, and ongoing support.
You do not need perfect certainty before making that first contact. You only need enough concern to ask better questions. If your loved one's mental health symptoms and substance use keep colliding, that is already enough reason to seek a full evaluation.
Hope usually doesn't arrive as a dramatic breakthrough. It often begins as a clear explanation, a coordinated plan, and one honest conversation.
If you're looking for answers, Casa Recovery offers a place to start with a confidential conversation about symptoms, treatment options, and insurance. Reaching out doesn't commit you to anything. It gives you a clearer picture of what help could look like.