You may be in a place many families know too well. A loved one is trying hard to get better, but every part of care feels split apart. The therapist talks about anxiety. The substance use counselor talks about drinking or pills. A psychiatrist may prescribe medication, but no one seems to be working from the same plan. Your family repeats the same painful history to each provider, and the person who needs help ends up carrying the burden of coordinating their own treatment.
That kind of care can leave people feeling blamed, confused, and exhausted. It can also miss the reality that mental health symptoms and substance use often feed each other. When that happens, treating one problem while sidelining the other rarely brings the stability a family is hoping for.
An integrated treatment approach is built for this exact situation. Instead of separating mental health care from addiction care, it brings them together into one coordinated process. For families looking at local options such as PHP, IOP, trauma therapy, and psychiatric support, understanding what integrated treatment looks like can make the search much less overwhelming.
Table of Contents
- The Challenge of Fragmented Care
- What Is an Integrated Treatment Approach
- Why Integration Is Essential for Co-Occurring Disorders
- The Integrated Pathway to Recovery in Action
- Hallmarks of a High-Quality Integrated Program
- Navigating Your Path at Casa Recovery
- Your Questions Answered and Next Steps
The Challenge of Fragmented Care
A common story sounds like this. A young man starts therapy for panic attacks, but he drinks every night to settle down enough to sleep. His therapist urges him to stop drinking because it worsens anxiety. His substance use counselor says he needs to get sober first before deeper trauma work can begin. His psychiatrist adjusts medication, but doesn't hear the full picture until weeks later.
Meanwhile, his family watches him bounce between providers who are all doing something helpful, but not together. He misses appointments, grows discouraged, and starts to believe treatment isn't working for him.
That is fragmented care. Each provider may be competent. The problem is the system around the person. Care becomes a set of separate conversations instead of one coordinated plan.
If you've ever wondered why this matters so much, it helps to understand how information is supposed to move across a care team. A plain-language resource on healthcare interoperability explained lays out why coordinated information-sharing is so important in healthcare generally. In behavioral health, that same principle matters even more because symptoms, triggers, medications, relapse patterns, and family dynamics are so closely linked.
What fragmentation looks like in real life
Families usually notice it before clinicians name it.
- Repeated intake stories: Your loved one tells the same painful history over and over.
- Mixed messages: One provider recommends trauma work now, another says wait.
- Medication blind spots: The prescribing clinician may not get timely feedback about cravings, sleep disruption, or side effects.
- Drop-offs during transitions: A person leaves residential treatment or crisis care and suddenly has to rebuild treatment from scratch.
When care is fragmented, the person in crisis often becomes the coordinator. That is too much to ask of someone already struggling.
An integrated treatment approach addresses this by bringing mental health and substance use treatment into one framework, with one team and one plan. For families, that usually feels less chaotic. For clients, it often feels more coherent, more respectful, and more possible.
What Is an Integrated Treatment Approach
An integrated treatment approach means mental health treatment and substance use treatment happen at the same time, through a coordinated team, inside the same overall plan of care. The point isn't just convenience. The point is clinical accuracy. If depression, trauma, anxiety, bipolar symptoms, or other psychiatric issues are interacting with substance use, treatment has to address the interaction, not just the separate labels.
What integrated really means
A clear definition comes from the Integrated Dual Disorder Treatment model. The Integrated Dual Disorder Treatment overview explains that this model mandates a stage-wise, multidisciplinary approach combining pharmacological management, psychotherapy, and family psychoeducation within a single service organization, with both conditions treated concurrently rather than sequentially.
That last phrase matters. Concurrently means no one says, "We'll deal with the trauma later," or "We'll only focus on sobriety for now," when both issues are actively shaping the person's daily functioning.
If you want a practical look at how this applies to dual diagnosis recovery, this guide on treating both mental health and addiction together gives a helpful local example.
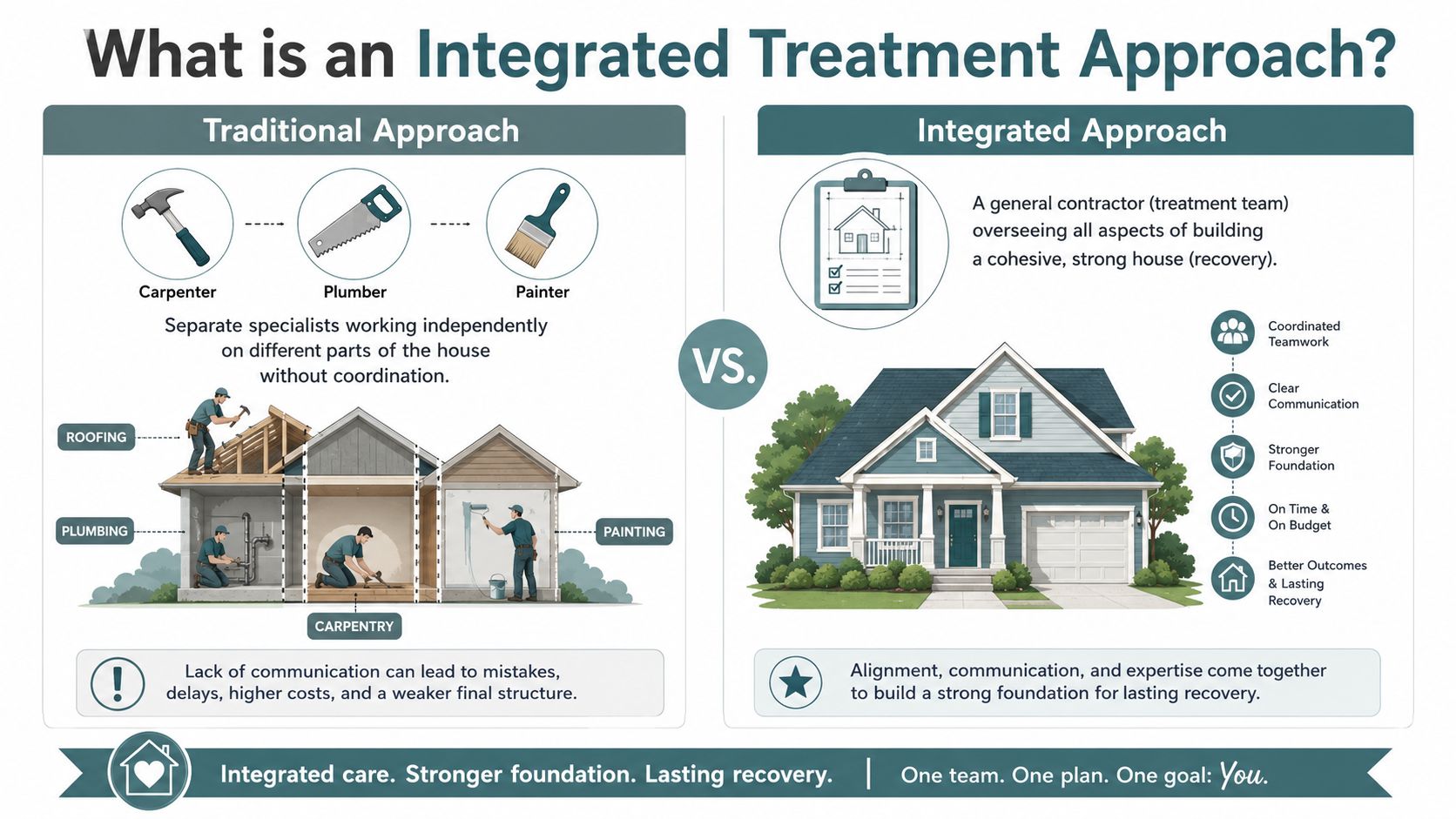
The house-building analogy
Think of recovery like building a house.
If you hire a plumber, electrician, and painter separately, without a shared blueprint or a general contractor, each person may do decent work. But problems show up fast. The painter finishes before wiring changes are complete. The plumber cuts into a wall that another worker just sealed. The project gets expensive, slow, and unstable.
Integrated treatment works like a general contractor model. The team shares one blueprint. Therapists, psychiatric providers, and addiction specialists coordinate timing, priorities, and goals. If anxiety spikes after early sobriety, the team adjusts. If trauma symptoms intensify, the treatment plan changes with that in mind. If medication is helping mood but affecting sleep or cravings, the clinicians can respond together.
Core principle: Treat the whole person, not isolated symptoms that happen to show up in different offices.
A strong integrated program doesn't just offer many services. It connects them so they reinforce each other.
Why Integration Is Essential for Co-Occurring Disorders
When people ask why integrated care matters so much, the short answer is this. Co-occurring disorders don't behave like separate problems. They interact. One condition can trigger, mask, worsen, or complicate the other.
Research shows that over 50 percent of people in the United States diagnosed with a severe mental illness also have a diagnosable co-occurring substance use disorder, which is one reason integrated service models are so important, according to this overview of integrated treatment program availability and need.

Why the cycle keeps going
Take anxiety and alcohol. Someone feels constantly keyed up, drinks to quiet their nervous system, then wakes in the night with worse anxiety as the alcohol wears off. The next day, they feel ashamed, exhausted, and more dependent on the same thing that is destabilizing them.
Trauma can work the same way. A person with intrusive memories, body tension, and emotional reactivity may use substances to numb those symptoms. But the numbing can interfere with sleep, relationships, work, and self-trust, which leaves trauma symptoms even more intense.
Depression can hide inside substance use, and substance use can hide inside depression. Families often ask, "Which came first?" Clinically, that isn't always the most useful question. The more urgent question is, "How are these problems keeping each other alive right now?"
For readers trying to understand how these conditions are documented in clinical settings, One For All Medical Billing's ICD-10 guide can be a useful reference. It won't tell you what treatment is best, but it does show how behavioral health conditions are classified in ways that affect evaluation, communication, and billing.
What the evidence tells us
A unified model has clear clinical advantages for psychiatric symptoms. A review published through PMC on integrated treatment outcomes found that integrated treatment for co-occurring disorders significantly improves psychiatric symptomatology, especially PTSD, anxiety, and depressive symptoms, with 54.5% of studies showing superior outcomes in that domain compared with non-integrated approaches.
That doesn't mean every symptom lifts quickly. It means the model is better aligned with how these disorders show up in human lives.
A local example of this kind of coordinated care is outlined in co-occurring disorder treatment in Orange County, where mental health and substance use needs are addressed together rather than split apart.
If one condition keeps triggering the other, treatment has to interrupt the whole cycle. Anything less leaves the engine running.
The Integrated Pathway to Recovery in Action
Families often understand the concept of integrated care, but still wonder what a real treatment path looks like day to day. In a high-quality outpatient setting, the process isn't random. It usually moves through structured levels of care that match how stable the person is, how intense symptoms are, and how much support is needed to function safely outside a residential setting.
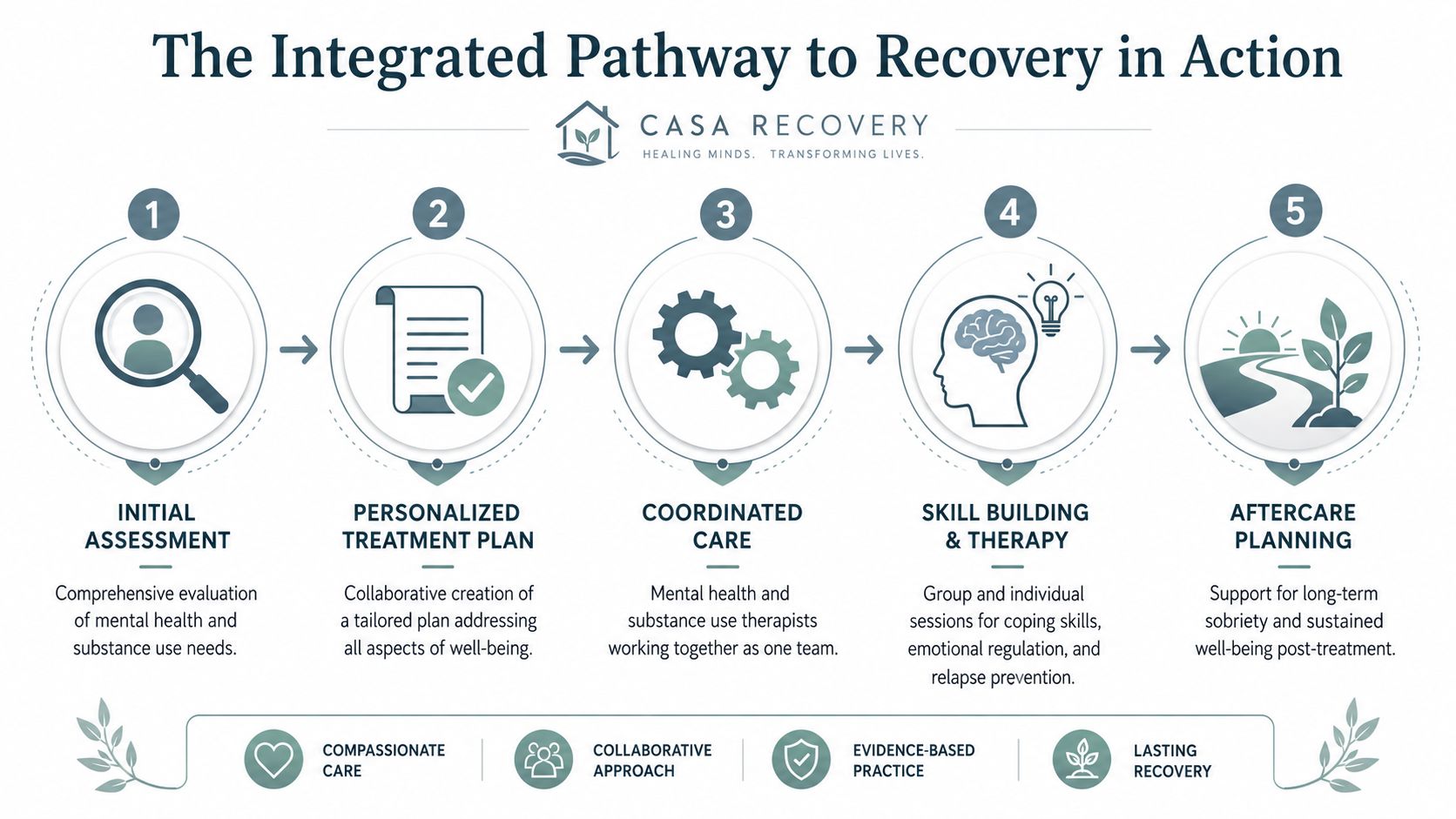
Starting with a full clinical picture
The first step is a thorough assessment. That means looking beyond the immediate crisis.
A good team asks questions such as:
- What symptoms are active right now: panic, depression, mood swings, trauma reactions, cravings, or sleep disruption.
- What role are substances playing: numbing, self-medication, binge patterns, withdrawal, or relapse triggers.
- What does the person need to function safely: structure, medication support, family involvement, supportive living, or step-down planning.
- What has and hasn't worked before: prior therapy, medications, treatment episodes, and transition failures.
This early assessment matters because integrated care isn't just "more services." It's a coordinated response to the patterns connecting symptoms and behavior.
How PHP and IOP work together
For many adults, Partial Hospitalization Program (PHP) is the right place to begin when symptoms are too disruptive for standard outpatient care, but inpatient hospitalization isn't necessary. PHP is often best understood as full-day structured treatment. The person spends much of the day in therapy, skills work, psychiatric follow-up, and recovery-focused programming, then returns home or to supportive living at night.
That structure can be especially helpful after residential treatment, after a psychiatric destabilization, or during an extended period of anxiety, depression, trauma activation, or relapse vulnerability.
Intensive Outpatient Program (IOP) is a step down in intensity. The client still receives robust care, but with fewer hours, which allows for gradual return to work, school, parenting, or other daily responsibilities.
A well-run integrated pathway uses those levels of care for different jobs:
| Level of care | What it helps with | What families often notice |
|---|---|---|
| PHP | Stabilization, routine, close observation, rapid treatment adjustments | Less chaos, better daily structure, faster feedback from the team |
| IOP | Practice in real life, continued therapy, relapse prevention, transition support | More independence with a safety net still in place |
The key isn't only that both levels exist. The key is continuity. The same clinical philosophy, and often the same core team, follows the person as care intensity changes. That reduces the "cliff" many clients feel when leaving a higher level of care.
Where EMDR and psychiatry fit in
Integrated treatment thus becomes tangible.
If trauma is driving both emotional instability and substance use, the plan may include EMDR within a broader therapeutic framework, rather than treating trauma as a separate issue to postpone indefinitely. If mood symptoms are severe, onsite psychiatry can evaluate medication needs while staying in close communication with therapists observing daily patterns in group and individual sessions.
That coordination changes practical decisions:
- A therapist notices that a client becomes highly dysregulated after family conflict.
- The psychiatric provider evaluates whether medication, sleep support, or timing adjustments are needed.
- The treatment team reinforces coping skills in groups and individual sessions.
- The client practices those skills while stepping down from PHP into IOP, instead of starting over with new providers.
Recovery tends to hold better when treatment intensity decreases gradually, not abruptly.
In a local integrated model, that often means psychiatry, trauma therapy, skills-based work, and dual-diagnosis support operate side by side rather than in separate silos.
Hallmarks of a High-Quality Integrated Program
A family often hears the word "integrated" and assumes it means everything is connected. Then they call a program and learn that therapy happens in one lane, psychiatry in another, and family support somewhere off to the side. A high-quality integrated program feels different in daily practice. The parts fit together the way a well-run medical team does, with each provider seeing the same person, the same risks, and the same treatment goals.
That difference becomes easier to spot when you know what to look for.
Trauma-informed care should show up in the structure
Many people with co-occurring disorders are carrying trauma, whether or not they have a formal trauma diagnosis. Some use substances to numb panic, shut down intrusive memories, or quiet a nervous system that stays on high alert. If treatment ignores that layer, the person may be asked to stop the coping strategy before they have learned a safer replacement.
A trauma-informed program does more than say the right words. The National Child Traumatic Stress Network outlines core trauma-informed principles such as safety, trust, collaboration, and attention to how trauma affects behavior and regulation. Those principles should be visible in the treatment design, not only in the marketing language.
In practical terms, families can look for signs like these:
- EMDR access: Helpful when trauma triggers, emotional flooding, and substance use are tightly linked.
- Trauma-focused options beyond talk therapy: Some clients need approaches that help with body-based distress or memories that are hard to put into words.
- Stabilization before trauma processing: Good care builds coping skills first, so clients are not pushed into material they are not ready to handle.
- One treatment plan for both issues: Trauma work and addiction treatment should inform each other instead of competing for attention.
For families comparing local options, this overview of co-occurring disorder support in South Orange County at Casa Recovery gives a clearer picture of how those pieces can be coordinated in one program.
Family work should be specific and structured
Families usually want to help. They often need guidance on how.
Good family programming teaches relatives what symptoms can look like, how relapse risk may show up at home, and how to respond without slipping into constant monitoring, conflict, or rescue patterns. That education is clinical care, not an extra courtesy.
A family program should not turn relatives into therapists. It should help them become informed, steady participants in recovery.
Home dynamics can support recovery, or they can stir up the same stress responses that feed both mental health symptoms and substance use. Clear boundaries, better communication, and realistic expectations give the client a better chance of practicing new skills outside the treatment setting.
Onsite psychiatry improves coordination
Medication decisions are more accurate when the psychiatric provider is part of the same treatment team that sees the client throughout the week. A therapist may notice rising anxiety after trauma work begins. Group staff may see sleep problems, irritability, or social withdrawal before the client names it directly. When psychiatry is onsite, those observations can shape the next clinical decision quickly.
Families can ask simple questions that reveal a lot:
- Does the psychiatrist communicate directly with therapists?
- Are medication changes discussed in the context of trauma history, substance use, and daily functioning?
- If a client is in PHP or IOP, does the psychiatric plan adjust with the intensity of care?
- Can the team explain how medications support the larger recovery plan?
Virtual care can also be part of a strong local program, especially for family meetings, check-ins, or selected clinical services. In those cases, privacy standards still matter. This overview of healthcare Zoom compliance is useful background for understanding what secure telehealth communication should include.
A strong integrated program is easier to recognize than it sounds. Trauma care is paced carefully. Family involvement has structure. Psychiatry is part of the conversation, not a disconnected referral. In a high-quality local model such as Casa Recovery, those details are what turn the clinical idea of "integrated treatment" into something a family can see, ask about, and trust.
Navigating Your Path at Casa Recovery
Once a family decides integrated care makes sense, the next hurdle is often emotional rather than clinical. People worry about saying the wrong thing on the first call. They worry they won't know whether symptoms are "serious enough." They worry about insurance, fit, and whether the program will understand co-occurring issues instead of flattening everything into one label.
That anxiety is normal. The first step should feel like a conversation, not an exam.
What happens on the first call
A strong admissions process starts by listening for the full picture. That includes mental health symptoms, substance use patterns, current safety concerns, prior treatment, medications, and what kind of support the family has right now.
This is also where practical questions get handled. The team can help with insurance verification, explain accepted PPO options and in-network relationships, and talk through whether PHP, IOP, or a mental health track appears to be the right level of care. If the caller is coming from outside the immediate area, supportive living coordination and logistics may also be part of the discussion.
Families who want a clearer sense of how that support can look locally can review how Casa Recovery supports co-occurring disorders in South Orange County.
What makes the experience feel different
The details matter here. A high therapist-to-client ratio and small group sizes can make treatment feel less anonymous. Individualized planning means the team isn't forcing every client into the same track. For clients with trauma histories, access to EMDR, Brainspotting, CBT, DBT, Motivational Interviewing, and psychiatric care in one coordinated setting can reduce the fragmentation that often derails progress.
What many families find reassuring is that the program can meet a person at different points in recovery. Some need the structure of PHP after a crisis or residential stay. Others are ready for IOP and focused on practicing recovery skills while resuming work, school, or family responsibilities.
The best admissions process doesn't pressure you. It helps you understand what level of care matches the person in front of you.
That transparency is often what lowers the temperature for families. Instead of trying to decode treatment on their own, they get a clearer path, concrete answers, and a sense that the program is looking for clinical fit rather than filling a spot.
Your Questions Answered and Next Steps
How do I know if integrated care is the right fit
A family often notices the pattern before they know the clinical term for it. Anxiety rises, substance use follows. Depression deepens, motivation drops, and treatment starts to feel like a revolving door. If both mental health symptoms and substance use are present, and each one keeps stirring up the other, integrated care is usually the model to look at first.
That is often the case when trauma, panic, depression, bipolar symptoms, relapse risk, or medication questions are all part of the same picture. Treating only one piece can leave the other active, much like repairing one side of a leaking roof while water is still getting in from the other.
What is the practical difference between PHP and IOP
PHP gives a person more structure, more clinical contact, and closer observation across the week. IOP still offers meaningful treatment, but with more room to keep up with work, school, or family responsibilities.
The choice is not about which level is "better." It is about which level matches the person in front of you right now. A high-quality local program should help families sort that out based on stability, symptom intensity, trauma history, daily functioning, and whether onsite psychiatric support may be needed early in care. At Casa Recovery, that also means looking at how therapies such as EMDR fit into the overall plan rather than treating trauma work as an afterthought.
Is there a fixed timeline for treatment
Usually, no.
Good care is adjusted to the person, not the calendar. Some clients need a longer period of stabilization before stepping down from PHP to IOP. Others gain traction more quickly and are ready for more independence sooner. Progress is best measured by readiness, consistency, and safety.
What should I look for when comparing programs
Look for signs that care is coordinated, not just listed on a website. Can the therapist, psychiatrist, and case manager communicate with each other? Is trauma treatment available in the same program if it becomes clinically appropriate? Does the program offer more than one level of care, so a client can step up or step down without starting over with a new team?
National guidance from SAMHSA describes integrated treatment for co-occurring disorders as care that addresses mental health and substance use conditions together, through coordinated services and a unified treatment plan. You can review that guidance in SAMHSA's resources on co-occurring disorders at samhsa.gov.
What is the next step if we are unsure
Start with a conversation. A good admissions call should lower confusion, not add pressure. The goal is to understand what has been happening, what level of care may fit, and whether the program can provide the kind of coordinated help your family has been missing.
If disconnected care has kept your family stuck, that does not mean recovery is out of reach. It often means the treatment approach has not matched the full problem yet.
If you're looking for compassionate, coordinated help in Orange County, Casa Recovery offers trauma-informed outpatient care for mental health and co-occurring disorders, including PHP, IOP, integrated dual-diagnosis treatment, onsite psychiatry, and family support. Reaching out for a confidential conversation can help you understand the right next step without pressure.