You might be reading this because someone you love has stopped functioning in ways that scare you. They aren't just stressed. They're missing work, crying for hours, not sleeping, not eating, or saying they can't do this anymore. Or maybe it's you, and the phrase “nervous breakdown” feels like the only words that match how far past your limit you've gone.
That phrase is common, but it also creates confusion. People use it to describe a real crisis, yet the label can make the situation sound vague, temporary, or less serious than it is. The most helpful shift is this one. A nervous breakdown isn't a medical diagnosis. It's a warning sign that something underneath, such as severe anxiety, depression, trauma-related symptoms, or another mental health condition, may need prompt professional care.
Table of Contents
- What Is a Nervous Breakdown (And What Is It Not)?
- Understanding the Causes and Triggers of a Breakdown
- Common Signs and Symptoms of a Mental Health Crisis
- What to Do Right Now for Safety and Stability
- How Professionals Diagnose and Treat a Breakdown
- A Guide for Family Members and Friends
- Frequently Asked Questions and When to Seek Emergency Care
What Is a Nervous Breakdown (And What Is It Not)?
When people ask what is a nervous breakdown, they're usually trying to make sense of a point where ordinary coping has stopped working. A person may feel emotionally flooded, mentally scattered, physically exhausted, and unable to do basic daily tasks.
The plain-language definition
A nervous breakdown is not a recognized medical diagnosis in the DSM-5 or ICD-11. Cleveland Clinic explains that it is a colloquial way to describe a severe mental health crisis in which stress, anxiety, or depression becomes so overwhelming that daily functioning breaks down (Cleveland Clinic on nervous breakdown).
That phrase “daily functioning” matters. It means the person may not be able to work, care for hygiene, think clearly, keep appointments, or stay engaged with other people. In clinical terms, the issue is less about the label and more about the functional collapse underneath it.
Practical rule: If someone can't reliably do the ordinary tasks that usually keep life moving, treat it as a mental health crisis, not “just stress.”
One way to think about it is a check-engine light. The light itself is not the engine problem. It tells you something underneath needs attention. “Nervous breakdown” works the same way. It points to distress, but it doesn't name the cause.
Stress can absolutely be part of the picture. If you want a simple breakdown of how normal pressure can become harmful overload, this overview of stress and how it affects the mind and body can help clarify the difference.
Why the label can mislead families
The phrase sounds familiar, which can make it seem less urgent than it is. Families often hear “breakdown” and assume the person needs rest, a few days off, or a chance to calm down. Sometimes rest helps. But when functioning has fallen apart, rest alone usually doesn't resolve the underlying condition.
People often get stuck by focusing on the word and missing the crisis. A better question isn't “Is this technically a nervous breakdown?” It's “What condition is showing up through this crisis, and how quickly does this person need support?”
That shift reduces shame. It also opens the door to proper care.
Understanding the Causes and Triggers of a Breakdown
A breakdown rarely comes out of nowhere. To family members, it can look sudden. To the person going through it, the collapse often follows a long period of strain, loss, fear, or untreated symptoms.
Houston Behavioral Healthcare notes that the term is often used for a severe crisis connected to untreated depression, anxiety, or chronic stress, and that approximately 26% of U.S. adults could experience a mental breakdown in their lifetime (Houston Behavioral Healthcare on causes, signs, and recovery). That matters because people in crisis often think, “Why am I the only one falling apart?” They aren't.
When stress keeps stacking up
Some people hit a crisis after months or years of running on empty. They may be juggling work pressure, caregiving, conflict at home, poor sleep, and the constant feeling that they have to keep pushing.
Then one more demand lands. A deadline. A breakup. A health scare. A financial shock. The person who seemed “fine” suddenly can't stop crying, can't focus, or can't leave bed. That doesn't mean they were fine before. It means their coping system was already overloaded.
People often call it a breakdown when what's really happened is this. The person's capacity ran out before the stress did.
Common trigger patterns
Several patterns show up again and again:
- Chronic stress: Long-term burnout, high-pressure work, caregiving strain, or relentless family conflict can wear down coping over time.
- Major life changes: Grief, divorce, job loss, moving, medical diagnoses, or trauma can push a vulnerable person into crisis.
- Untreated mental health symptoms: Anxiety, depression, trauma-related symptoms, mood instability, or panic may build gradually until functioning drops sharply.
- Isolation: People who stop talking about what they're carrying often look stable right up until they aren't.
- Substance use complicating the picture: Alcohol or drugs may seem like a way to calm down or sleep, but they can intensify mood swings, anxiety, and impaired judgment.
Families also get confused because the cause is not always one dramatic event. Sometimes the trigger is cumulative. The person didn't “overreact” to one thing. They reached the end of what they could absorb.
Common Signs and Symptoms of a Mental Health Crisis
A nervous breakdown can look different from person to person, but it often reflects severe anxiety or depression. One source cited in your brief notes that in the U.S. 1 in 8 adults regularly reports feelings of worry or anxiety, and 2 in 5 high school students reported depression symptoms in 2023 (Nature-linked summary in provided data). The point isn't to blur everyday stress with crisis. It's to show that the conditions underneath a breakdown are common, real, and medically significant.
What symptoms can look like day to day
It helps to group symptoms by how they show up.
- Emotional signs: Intense sadness, panic, hopelessness, sudden irritability, uncontrollable crying, or feeling emotionally numb.
- Cognitive signs: Racing thoughts, poor concentration, indecision, feeling detached, catastrophic thinking, or fear that something terrible is about to happen.
- Physical signs: Exhaustion, shaking, chest tightness, insomnia, sleeping most of the day, appetite changes, nausea, or feeling constantly “on edge.”
- Behavioral signs: Withdrawing from people, missing work, neglecting hygiene, staying in bed, not answering calls, or being unable to complete simple tasks.
Many families ask whether these are “real symptoms” or just signs the person needs to try harder. They are real symptoms. When anxiety is severe, attention narrows and the body stays in alarm mode. When depression deepens, even basic tasks can feel impossible.
If racing thoughts are making it hard to settle enough to eat, sleep, or think clearly, some people find it useful to learn strategies to manage racing thoughts while they're arranging formal help. That kind of tool is not a substitute for care, but it can help lower the temperature in the moment.
Anxiety symptoms can be especially confusing because they affect the body as much as the mind. This guide to signs and symptoms of anxiety may help you recognize when “stress” is crossing into something more serious.
Nervous Breakdown Misconceptions vs. Clinical Reality
| Common Misconception | Clinical Reality |
|---|---|
| A nervous breakdown is a formal diagnosis. | It's a common phrase, not a clinical diagnosis. Professionals look for the underlying condition. |
| It means the person is weak. | It means coping has been overwhelmed. That can happen when symptoms and stress outpace support. |
| If they sleep for a few days, they'll bounce back. | Rest can help, but persistent loss of functioning often needs professional assessment and treatment. |
| It's just dramatic anxiety. | Severe anxiety can be disabling. So can depression, trauma-related symptoms, and mood episodes. |
| If they can text or smile, it can't be serious. | People in crisis can still mask symptoms for short periods. Functioning over time matters more than a brief moment. |
| Talking about help will make it worse. | Calm, direct support often reduces isolation and helps the person move toward care. |
What to Do Right Now for Safety and Stability
When someone is in the middle of a crisis, clarity helps more than long explanations. Focus on safety, slowing things down, and bringing in support.
Immediate steps to lower risk
Move to a calmer place. Reduce noise, conflict, and stimulation. A quiet room with one supportive person is usually better than a crowd asking questions.
Stay with one simple goal. Don't try to solve work, relationships, or long-term decisions right now. The goal is to get through this moment safely.
Contact one trusted person. Ask someone steady to come over, stay on the phone, or help with next steps. A person in crisis shouldn't have to organize help alone.
Use direct language about safety. Ask clearly if they're thinking about hurting themselves or if they feel unable to stay safe. Calm questions do not “put the idea” in someone's head.
Call or text 988 if there is suicidal thinking, self-harm risk, or you're not sure how serious it is. The verified data in your brief states that the 988 Suicide & Crisis Lifeline is critical for individuals with self-harm ideation.
Delay major decisions. Don't quit a job, end a relationship, empty accounts, or make major moves in the middle of a breakdown state.
Try grounding, not debate. Have them name five things they see, four they feel, three they hear, two they smell, and one they taste. This can reduce overwhelm enough to take the next step.
If someone says they don't feel safe with themselves, believe them and shift immediately into crisis support.
If the person is becoming more disorganized, more agitated, or less able to care for basic needs, treat that as escalating risk.
How Professionals Diagnose and Treat a Breakdown
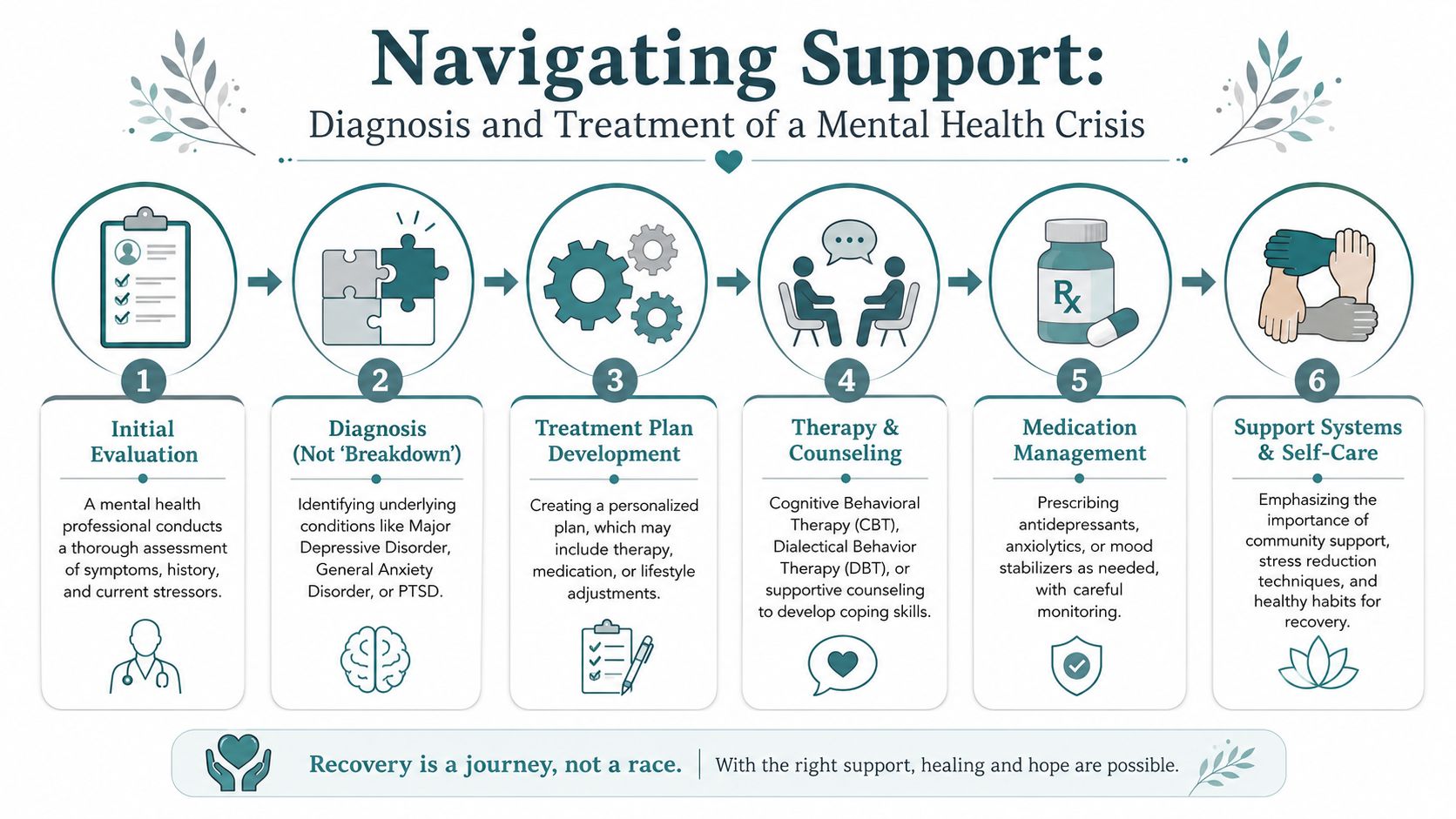
Clinicians don't diagnose “nervous breakdown.” They assess the symptoms, functioning, history, current stressors, and safety concerns to identify what condition or conditions are driving the crisis.
What an evaluation usually focuses on
A good assessment often explores several questions:
- What has changed recently: sleep, appetite, mood, energy, work functioning, substance use, or social withdrawal.
- Whether there are immediate safety risks: self-harm thoughts, suicidal thinking, violence risk, or inability to meet basic needs.
- What diagnosis may fit best: depression, an anxiety disorder, trauma-related symptoms, bipolar disorder, panic symptoms, or co-occurring substance use.
- How much structure is needed right now: standard outpatient care, a more intensive day program, urgent crisis services, or emergency care.
This is why the gap between the everyday phrase and the clinical reality matters. The label is broad. Treatment has to be specific.
Some families also want a clearer sense of what counseling options can look like in real life before making calls. If that would help, this overview of understanding Penticton counselling choices gives a simple example of how people compare support options and levels of care.
What treatment can include
Healthdirect states that treatment targets the underlying condition and may include SSRIs or SNRIs, while benzodiazepines may be used short-term for acute anxiety. The same verified source notes that recovery is often established at 4 to 6 weeks after diagnosis and treatment initiation, though the exact course depends on the condition being treated (Healthdirect on treatment and recovery).
Medication is only one part of care. Therapy often does the day-to-day rebuilding.
- Cognitive Behavioral Therapy (CBT): Helps a person identify thought patterns, avoidance habits, and stress responses that keep the crisis going.
- Dialectical Behavior Therapy (DBT) skills: Can help with emotional regulation, distress tolerance, and impulsive reactions.
- Trauma-focused therapies: Approaches such as EMDR or Brainspotting may be considered when unresolved trauma is contributing to panic, shutdown, or repeated overwhelm.
- Structured outpatient care: Some people need more than a weekly appointment. Partial Hospitalization Programs (PHP) or Intensive Outpatient Programs (IOP) offer a higher level of support when someone is too unstable for standard outpatient therapy but does not need inpatient hospitalization.
- Psychiatric follow-up: Ongoing monitoring helps adjust medication and track changes in sleep, mood, anxiety, and functioning.
For a deeper look at therapeutic approaches commonly used in mental health care, this guide on psychological treatments for mental health is a useful overview.
The right treatment plan answers two questions at once. What diagnosis best explains the crisis, and what level of care will restore stability safely?
A Guide for Family Members and Friends
Families often feel helpless because they can see the crisis but can't fix it. Your role isn't to diagnose or force a breakthrough conversation. Your role is to lower shame, increase safety, and help the person connect with care.

Mayo Clinic's guidance, as summarized in the verified data provided, notes that professionals no longer use the term “nervous breakdown” and instead diagnose underlying conditions such as depression or anxiety. That misunderstanding can delay care and makes it important for families to recognize the situation as a medical crisis that may require interventions such as PHP or IOP (Mayo Clinic FAQ on the term nervous breakdown).
What helps in the moment
Try language that is simple and grounded:
- “I'm here with you.” That reduces isolation.
- “You don't have to explain everything right now.” That lowers pressure.
- “I'm worried because you don't seem able to function the way you usually do.” That focuses on what you're seeing, not blame.
- “Let me help you make one call.” Specific help works better than “Let me know if you need anything.”
You can also help with logistics. Offer to sit with them while they call a therapist, crisis line, doctor, or program. Drive them to an appointment. Help write down symptoms. Handle practical details if they're too overwhelmed to organize.
What not to say
Avoid phrases that sound motivating but land as dismissive.
- “Just calm down.”
- “Everyone gets stressed.”
- “Be grateful.”
- “You're overthinking this.”
- “Other people have it worse.”
These responses often increase shame and make the person less likely to be honest about risk.
“I believe you're struggling” is often more useful than “Why can't you snap out of it?”
Family members also need support. If you're helping someone in crisis, take turns, stay in communication with other trusted adults, and don't carry the whole situation by yourself.
Frequently Asked Questions and When to Seek Emergency Care
A nervous breakdown can sometimes be managed with urgent outpatient support. Sometimes it crosses into emergency territory. You need a clear line between the two.
When it is an emergency
Call 911 or go to the nearest emergency room if the person has:
- An active suicidal plan or recent suicide attempt
- Threats or intent to seriously harm someone else
- Psychosis, such as hallucinations, delusions, or extreme confusion
- An inability to care for basic needs, such as eating, drinking, hygiene, or staying physically safe
- Severe disorientation or behavior that makes immediate harm more likely
If you're unsure whether it's “serious enough,” err on the side of safety. Crisis states can change quickly.
Common questions about recovery
Can someone fully recover?
Yes. Recovery is possible, especially when the underlying condition is identified and treated rather than minimized.
How long does recovery take?
It depends on what is driving the crisis, how long symptoms have been building, and how quickly treatment starts. Some people stabilize relatively quickly. Others need a longer period of structured support.
Is a nervous breakdown the same as burnout?
Not exactly. Burnout can be part of the path into crisis, but a breakdown usually means functioning has fallen much further.
Will the person need medication?
Maybe. Some people do well with therapy alone. Others benefit from medication, especially when anxiety, depression, panic, or mood instability is severe.
Do they need a higher level of care?
If they can't function reliably, keep themselves safe, or follow through with ordinary outpatient appointments, a more structured level of care may be the safer option.
If you're trying to sort out what kind of support fits the situation, an admissions team can often help you understand the difference between outpatient therapy, intensive outpatient care, and emergency services.
If you or someone you love is in Orange County and struggling with what feels like a nervous breakdown, Casa Recovery provides trauma-informed mental health and dual-diagnosis care for adults, including PHP, IOP, psychiatric support, and family involvement. If you're unsure what level of care makes sense, reaching out for guidance can be a practical first step toward safety and stabilization.