You're probably looking at treatment websites right now and seeing the same words over and over. Personalized care. Compassionate team. Evidence-based therapies. Dual diagnosis. It all starts to blur together, especially when you're worried, tired, and trying to make a decision that feels urgent.
That confusion is normal. Families often assume that if two programs both say they offer CBT, DBT, medication management, or trauma therapy, they must be roughly the same. They aren't. The biggest difference is often not what a center lists on its website, but how those services are delivered.
Evidence based addiction treatment is the clearest signal to look for, but only if you understand what the phrase means in real clinical practice. It doesn't mean trendy language. It means care built on methods that have been studied, applied by trained clinicians, and adapted to the person in front of them. When you know how to spot that difference, the search becomes far less overwhelming.
Table of Contents
- Introduction Navigating the Path to Recovery
- What Evidence Based Really Means for Addiction Recovery
- The Core Therapies in Evidence Based Treatment
- Why Dual Diagnosis and Trauma-Informed Care Are Essential
- The Proven Outcomes of Evidence Based Treatment
- How to Evaluate an Addiction Treatment Program
- Finding Evidence Based PHP and IOP in Orange County
Introduction Navigating the Path to Recovery
Searching for addiction treatment can feel like trying to make sense of a foreign language under pressure. You're asked to compare levels of care, therapy names, medication options, and mental health services, often while a loved one is in crisis or barely willing to accept help.
The good news is that there is a practical way to sort through the noise. Start by asking whether a program provides evidence based addiction treatment, then go one step further and ask whether it delivers those therapies with quality and consistency. That second question is where many families miss the mark.
A program can sound clinically advanced and still provide shallow, inconsistent care. A stronger program will be able to explain what it does, why it does it, how often it does it, and how treatment is matched to the person's actual needs.
What Evidence Based Really Means for Addiction Recovery
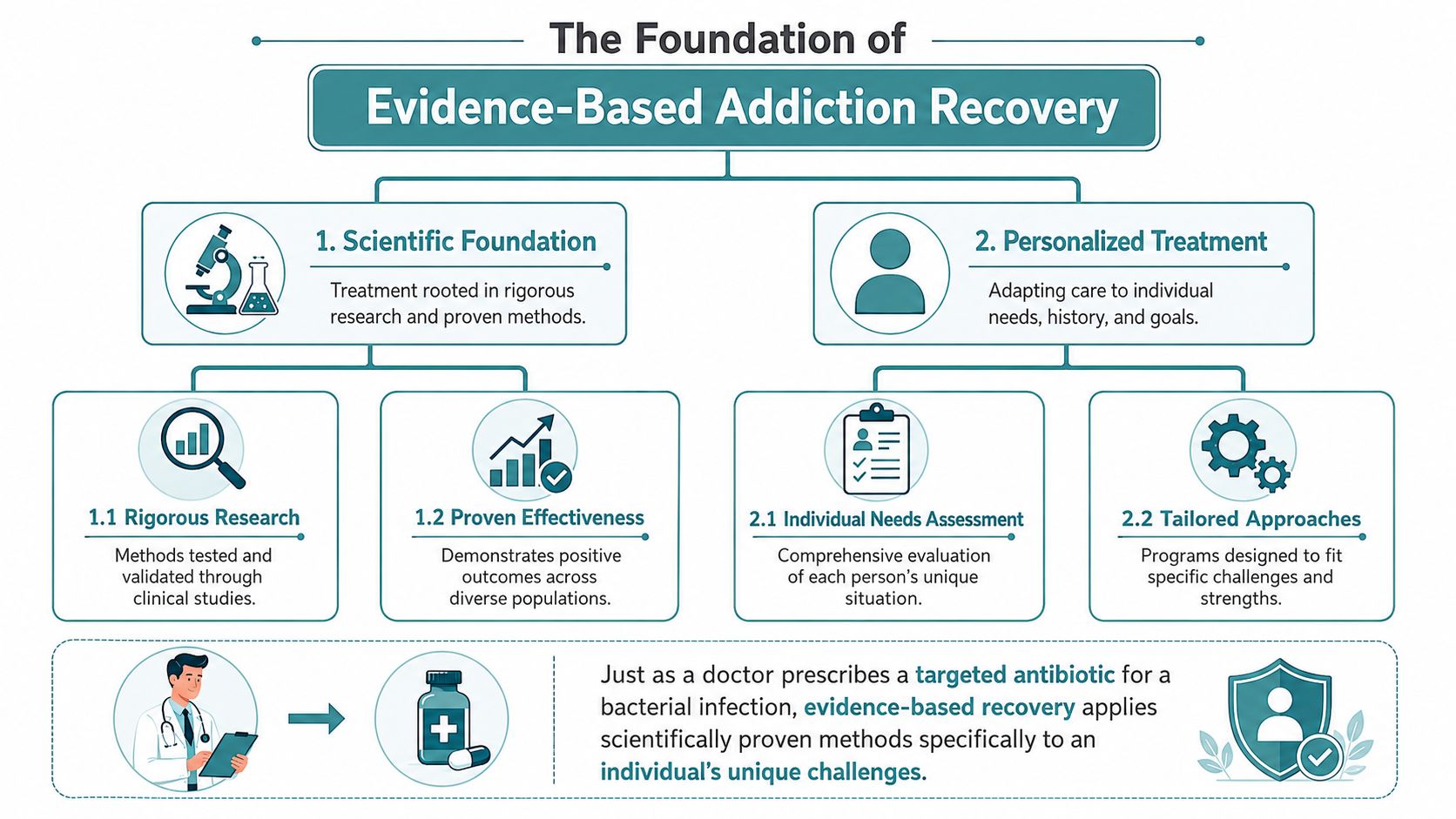
Evidence based care isn't a single therapy. It's a way of making treatment decisions. The simplest analogy is medical care for an infection. A physician doesn't choose treatment based on what sounds comforting or what was popular years ago. They use approaches that have been tested, then adjust them based on the patient's condition, history, and risks.
That same logic applies to addiction treatment. The goal isn't to throw a list of services at someone. The goal is to choose interventions with a scientific foundation and fit them to the individual.
Why the term matters
Many people hear “evidence based” and assume it means rigid or impersonal. In good treatment, it means the opposite. It means clinicians aren't relying on guesswork, slogans, or a one-size-fits-all model.
It also means treatment can adapt when abstinence isn't the only immediate goal. Federal guidance on low-barrier models emphasizes that effective care for complex addiction may include flexible scheduling, non-punitive responses to ongoing use, and harm reduction strategies to support retention and reduce overdose risk, as described in SAMHSA's advisory on low-barrier models of care.
Practical rule: If a program uses “evidence based” to mean “everyone gets the same formula,” that's a warning sign, not a strength.
The three parts of real evidence based care
A reliable program balances three things at once:
Research
The treatment methods themselves should be supported by established addiction science. That includes therapies and medications shown to help with retention, symptom reduction, and recovery outcomes.
Clinical expertise
Research doesn't treat people. Clinicians do. A strong therapist or prescriber knows when to use a modality, when to pause, and when a patient needs more structure, more psychiatric support, or a different pace.
Patient values and needs
Recovery works better when care fits the person's life. That includes their substance use history, trauma history, mental health symptoms, family system, motivation level, medical needs, and practical barriers like work or childcare.
This is why the phrase matters so much. Evidence based addiction treatment isn't just about which therapies appear in a brochure. It's about whether a team can connect science, judgment, and personalization in a way that helps someone stay engaged.
The Core Therapies in Evidence Based Treatment
A family calls a treatment center and hears a reassuring list: CBT, DBT, motivational interviewing, trauma therapy, medication support. On paper, that can sound excellent. The harder question is whether those therapies are delivered the way they were designed to work, by trained clinicians, in the right sequence, and for the right patient.
That is the gap families miss all the time. A center can list evidence-based therapies on a website and still provide uneven care if those methods are used loosely, applied to everyone the same way, or offered without enough staff training and supervision.
A strong program uses different therapies for different jobs. The therapies below are not interchangeable. They work more like tools in a well-stocked workshop. You would not use a wrench to do a saw's job, and you would not expect one therapy to solve craving, trauma, emotion regulation, and ambivalence all at once.
What each therapy is designed to do
Cognitive Behavioral Therapy, or CBT, helps a person identify the chain that links a trigger to substance use. That chain might look like stress, then hopeless thoughts, then isolation, then craving, then use. CBT teaches people to interrupt that sequence with more accurate thinking and specific coping responses. In a quality program, CBT is not just "talking about your week." It includes practice, review, and skills applied to real relapse patterns.
Dialectical Behavior Therapy, or DBT, helps people who feel emotions intensely and act quickly under stress. It teaches distress tolerance, emotion regulation, mindfulness, and relationship skills. For someone whose substance use is tied to panic, anger, self-harm, or repeated blowups with loved ones, DBT can create enough stability for recovery work to hold.
Motivational Interviewing, or MI, is often misunderstood because it can sound simple. It is a structured counseling style that helps people work through ambivalence instead of arguing with them about change. According to SAMHSA's guidance on motivational interviewing, MI is widely used to improve engagement and strengthen a person's own reasons for treatment. In practice, that means a skilled clinician knows how to lower defensiveness without becoming passive.
Contingency Management uses positive reinforcement to support recovery behaviors such as attendance, participation, and drug-free testing when that fits the treatment plan. Families sometimes hesitate here because rewards can sound childish or superficial. In behavioral treatment, consistent reinforcement works much like physical therapy after an injury. Repetition and feedback help a new behavior become more likely the next time stress hits.
Medication for addiction treatment can be life-protective, especially for opioid and alcohol use disorders. Medications such as buprenorphine and methadone help stabilize opioid use disorder and reduce overdose risk, as described by NIDA's overview of medications to treat opioid use disorder. A program's real stance on evidence often becomes clear here. If a center advertises evidence-based care but discourages appropriate medication for philosophical reasons, families should ask hard questions.
Trauma-focused therapies, including EMDR and Brainspotting, can help when trauma is part of the addiction cycle. Timing matters. Trauma work should follow adequate stabilization, safety planning, and support for co-occurring symptoms. Programs that rush into trauma processing without enough grounding can overwhelm patients instead of helping them.
Delivery matters as much as the label.
A center may say it offers DBT, for example, but only provide a few generic coping worksheets. It may claim trauma-informed care while using confrontational practices that leave patients feeling exposed or shamed. It may list MI on a brochure while staff rely on persuasion and pressure in sessions. Families should listen for signs that a therapy is being used with structure and fidelity, not just named for marketing value.
One practical way to check is to ask how the therapy is delivered. Is CBT part of an individualized treatment plan with homework and review? Is DBT taught by clinicians trained in the model? Is medication integrated with therapy and psychiatric care, or treated as separate? Is trauma work paced carefully, with attention to safety and stabilization, along with effective coaching practices for safety and clear clinical boundaries?
For a practical example of how these methods may be combined in actual care, this overview of therapeutic modalities in addiction and mental health treatment shows how multiple clinical approaches can be used together rather than presented as isolated buzzwords.
Key Evidence-Based Addiction Therapies at a Glance
| Therapy | Primary Focus | Best For |
|---|---|---|
| CBT | Changing harmful thought and behavior patterns | Relapse prevention, cravings, depression, anxiety, distorted thinking |
| DBT | Managing intense emotion and improving relationships | Emotional dysregulation, impulsivity, self-destructive behavior |
| MI | Strengthening internal motivation for change | Early engagement, ambivalence, resistance to treatment |
| Contingency Management | Reinforcing healthy recovery behaviors | Attendance, consistency, behavior change support |
| Buprenorphine or Methadone | Stabilizing opioid use disorder and reducing overdose risk | Opioid use disorder, especially when relapse and overdose risk are high |
| Trauma-focused therapies such as EMDR or Brainspotting | Processing trauma within a structured treatment plan | People with trauma histories contributing to substance use |
Why Dual Diagnosis and Trauma-Informed Care Are Essential
Many families still think of addiction as the main problem and anxiety, depression, trauma, or mood swings as secondary issues. In practice, those conditions are often tightly woven together. Someone may drink to shut down panic, use stimulants to push through depression, or rely on opioids after years of unresolved trauma and emotional pain.
Why treating only the addiction falls short
If a program tries to “get the substance use under control first” and postpones mental health treatment, the person often returns to the same drivers that kept the addiction going. You can remove the substance for a short time without changing the conditions that made it feel necessary.
Integrated dual-diagnosis care treats both conditions at the same time. That means the same team is looking at mood symptoms, anxiety, trauma reactions, sleep, medication needs, craving patterns, family stress, and daily functioning as one clinical picture. This is the standard families should expect, not an extra feature.
For a more detailed explanation of how this works, this resource on understanding dual diagnosis and treating mental health and addiction together gives a useful overview of why integrated care supports more durable recovery.
What trauma-informed care looks like in practice
Trauma-informed care doesn't mean every session is trauma processing. It means the entire program is built around safety, predictability, collaboration, and respect. Staff understand that shame, defensiveness, avoidance, numbness, and anger may be protective responses, not character flaws.
That changes how clinicians speak to patients, how groups are run, how setbacks are handled, and how quickly a person is pushed into emotionally intense work. Families who want a broader perspective on safety-centered support may also find these effective coaching practices for safety helpful, because they illustrate principles that overlap with trauma-informed clinical environments.
A person who doesn't feel safe rarely stays open long enough to benefit from treatment.
Programs that aren't trauma-informed may still use the right therapy names. The experience can still feel harsh, shaming, or destabilizing. That disconnect matters. Clinical quality isn't only about what intervention is listed. It's also about whether the environment allows the intervention to work.
The Proven Outcomes of Evidence Based Treatment
A family often reaches this point with a practical question. If two programs both say they use evidence-based treatment, will the outcomes really be different?
Sometimes, yes. The difference is not the label. The difference is whether the treatment is delivered consistently, by trained clinicians, for long enough, and in a plan that matches the person in front of them. A recipe only works if someone follows it. Addiction treatment works the same way.
Why length of care matters
One finding has shaped addiction treatment for decades. People tend to do better when care lasts long enough for new habits, coping skills, and clinical stability to take hold. A brief detox can help someone get physically safe, but it does not usually give enough time to rebuild daily routines, address triggers, repair judgment, and stabilize co-occurring symptoms. A historical review of evidence-based treatment research explains why longer engagement became such an important part of modern care planning.
This can be hard for families to hear, especially after a crisis. Many people hope one short stay will fix the problem. More often, recovery works like physical rehabilitation after a serious injury. The first stage gets the person out of immediate danger. The next stage is where strength, repetition, and lasting function are built.
Why well-delivered treatment gets better results than fragmented care
Research on extended care has linked longer, structured treatment and follow-up with better substance use outcomes. Studies have also found that combining behavioral therapies with medication can outperform a pieced-together approach or medication alone, as noted earlier. The pattern is consistent. Treatment tends to work better when it is organized, sustained, and matched to the person's needs.
That point matters because many centers advertise the right therapies. The stronger programs deliver them in a way that patients can effectively use. A patient who receives regular CBT with clear goals, skill practice, and progress review is getting something very different from a patient who sits in a loosely structured group that borrows the CBT label. On paper, those programs may look similar. In real life, the outcomes can separate quickly.
Recovery usually improves through sustained, well-delivered care, not through a short burst of stabilization alone.
Families do not need to become researchers to understand this. They just need to ask a better question. Instead of "Do you offer evidence-based treatment?" ask "How do you deliver it, how often, by whom, and for how long?" That is often where the gap between marketing and clinical quality becomes clear.
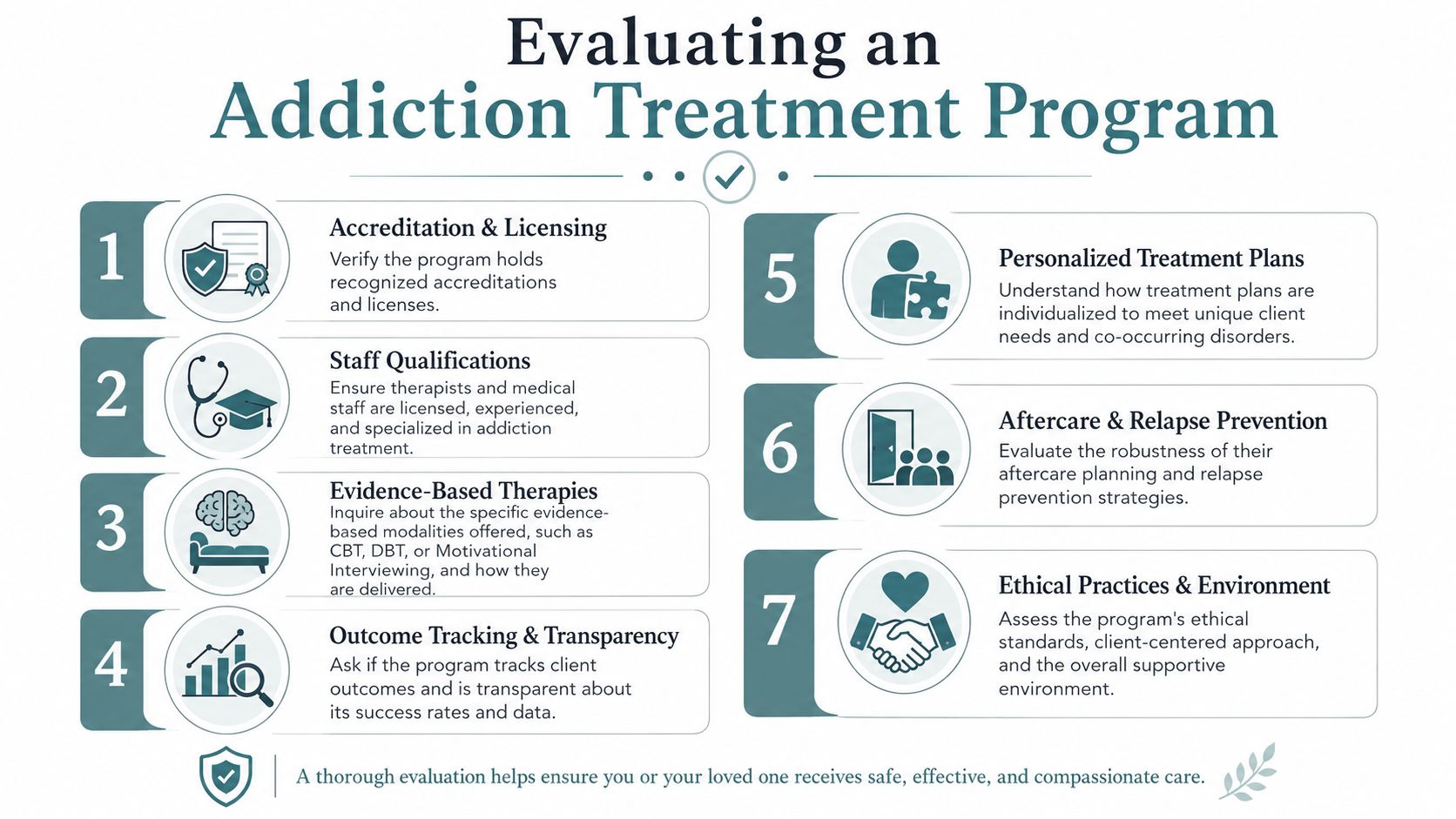
How to Evaluate an Addiction Treatment Program
Families can protect themselves from polished marketing. A center may accurately say it offers CBT, DBT, MI, trauma work, psychiatry, or relapse prevention. The harder question is whether those services are delivered with enough quality and consistency to make a difference.
The field has a known problem with low-fidelity implementation, meaning therapies may be widely advertised without being delivered according to the standards that made them effective in the first place, as discussed in the National Academies overview of psychosocial interventions and implementation challenges. In plain terms, the therapy name alone doesn't tell you much.
How to spot the fidelity gap
The simplest example is CBT. One program may provide structured individual CBT sessions with clear goals, homework, behavioral planning, and progress review. Another may call a general supportive conversation “CBT” because a licensed therapist led the session. Those aren't equivalent forms of care.
The same problem happens with DBT. True DBT-informed work has specific skills and a recognizable structure. If a center says it offers DBT but can't explain how skills are taught, practiced, and reinforced, the label may be doing more work than the treatment itself.
Questions families should ask before enrolling
Ask direct questions and listen for specific answers.
- Ask about frequency: How many individual sessions will the patient receive each week, and what kind of therapy happens in those sessions?
- Ask about integration: How are substance use, mental health symptoms, trauma history, and medication needs coordinated in one treatment plan?
- Ask who provides care: Are therapists licensed? What specific training do they have in the modalities the center lists?
- Ask for the weekly schedule: A real schedule tells you more than a brochure. You can see structure, intensity, and whether the day is clinically meaningful.
- Ask how progress is reviewed: How does the team know when treatment is working, when it needs adjustment, or when a higher or lower level of care is needed?
- Ask how setbacks are handled: Does the program respond to relapse or return to use with engagement and reassessment, or with punishment and discharge?
You're also watching how the admissions team responds. A solid program usually welcomes these questions. Vague answers, defensiveness, or pressure to commit quickly should make you slow down.
One useful test is this. Replace “Do you offer CBT?” with “How is CBT used in this person's plan, who delivers it, and what would I expect to see on the schedule?” The first question invites a yes. The second reveals quality.
Finding Evidence Based PHP and IOP in Orange County
For many adults in Orange County, the most realistic form of high-quality care is outpatient treatment with real structure. That usually means PHP or IOP. These programs let people receive coordinated therapy, psychiatry, skills work, and family support while staying connected to daily life and practicing recovery in the real world.
What strong outpatient care should include
Good PHP and IOP programs reduce the risk of fragmented treatment by keeping the same clinical team involved over time. Recent guidance highlighted the value of continuous engagement, including step-down supports such as PHP and IOP, to avoid the rebound that often follows short, disconnected episodes of care, as described in this discussion of evidence-based SUD treatment for young adults.
In practical terms, families in Orange County can look for outpatient programs that offer integrated dual-diagnosis treatment, trauma-informed care, medication management, and meaningful individual therapy rather than group-only programming. If a person needs step-down support after residential treatment or needs more structure than standard weekly therapy, an Intensive Outpatient Program for substance abuse may be one appropriate option to explore.
One Orange County example is Casa Recovery, a San Juan Capistrano program that provides PHP and IOP with integrated dual-diagnosis care, onsite psychiatry, trauma-informed treatment, family involvement, and therapies such as CBT, DBT, EMDR, Brainspotting, and Motivational Interviewing. What matters most isn't the list alone, but whether the structure, staffing, and coordination support consistent delivery across the full course of care.
If you're trying to decide what kind of help makes sense for you or someone you love, Casa Recovery offers outpatient mental health and dual-diagnosis treatment in Orange County, including PHP and IOP, with admissions guidance and insurance verification.