If you're searching for PHP near me after a loved one has been placed on a 5150 hold, you're probably exhausted, scared, and trying to make decisions fast. Most families reach this moment with very little preparation. One day you're managing a crisis at home, in the ER, or after a call from law enforcement. The next, you're hearing unfamiliar terms and trying to figure out what happens after the immediate danger passes.
This is the part many people aren't prepared for. A 5150 is about emergency safety. It isn't a long-term recovery plan. Once the hold ends, people often need a structured next step that offers more support than weekly therapy, but less restriction than staying in a hospital. That's where a Partial Hospitalization Program, or PHP, often fits.
A good PHP can become the bridge between crisis and steadier daily life. It gives someone a place to keep receiving care, build routines, practice coping skills, and stay closely connected to clinicians while sleeping at home each night.
Table of Contents
- What Is a 5150 Psychiatric Hold in California
- Patient Rights During a 72-Hour Hold
- After 72 Hours Discharge and Extension Options
- The Bridge to Recovery Partial Hospitalization Programs PHP
- How PHP Prevents Re-Hospitalization and Builds Stability
- Finding Hope and Healing at Casa Recovery
- Your Immediate Next Steps to Getting Help
What Is a 5150 Psychiatric Hold in California
What PHP means in mental health
Before going further, it helps to clear up one common point of confusion. In mental health, PHP means Partial Hospitalization Program. It has nothing to do with computer programming. When families search for PHP near me, they're usually looking for a high level of outpatient support after a psychiatric crisis.
A 5150 hold in California is an emergency psychiatric hold used when trained professionals believe a person is in immediate danger because of a mental health crisis. In plain language, it's a short-term safety measure. It isn't meant as punishment, and it doesn't mean someone has failed.
This image helps show the basic flow.
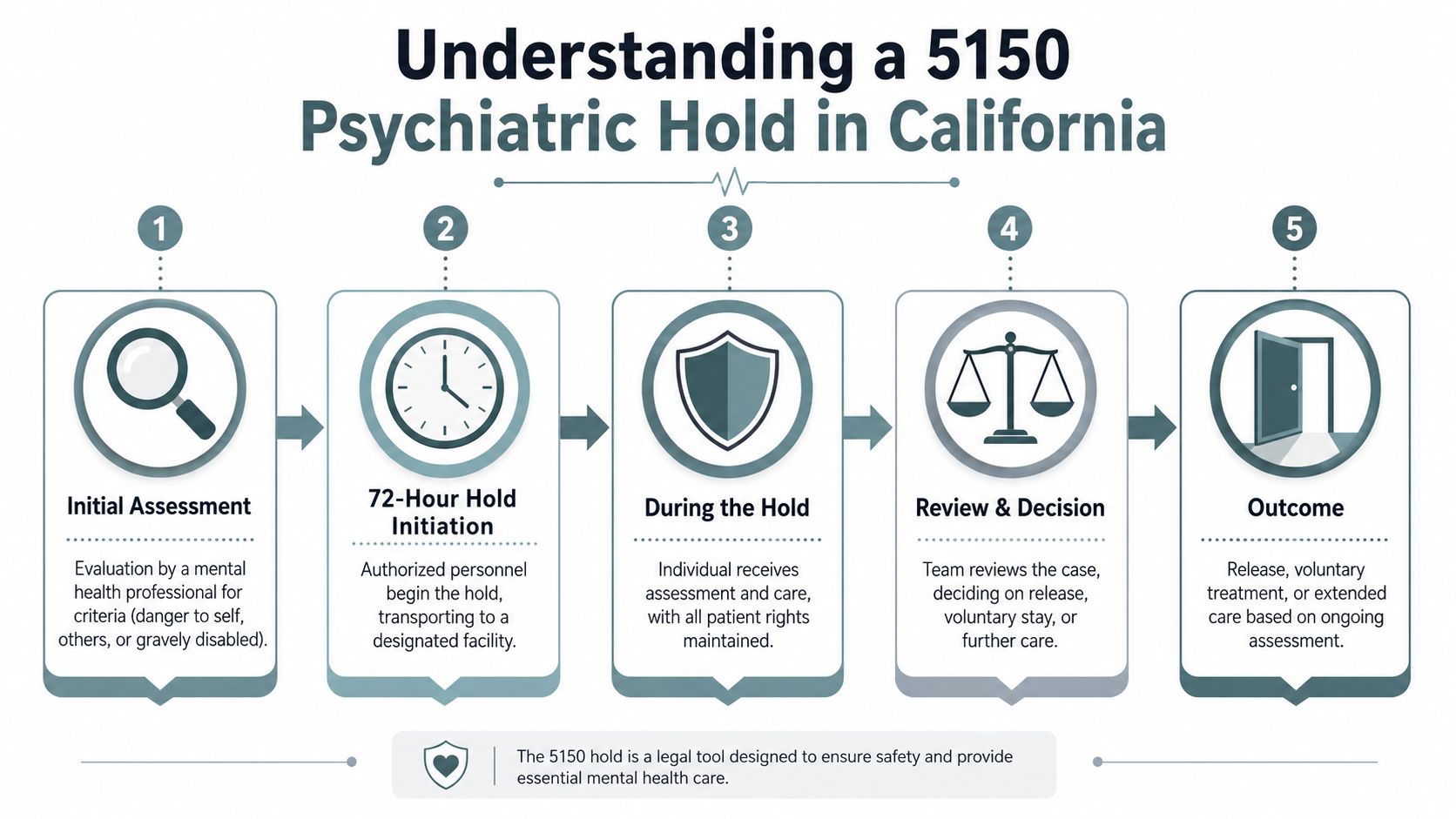
Families often hear “72-hour hold” and assume the process is simple and automatic. It usually doesn't feel simple to the person in crisis or to the people who love them. Evaluations, observation, and decisions about next care all happen during a very stressful period.
The three reasons someone may be placed on a 5150
A 5150 generally centers on three concerns:
- Danger to self: This can include suicidal thinking, suicidal actions, or behavior that suggests the person may seriously harm themselves.
- Danger to others: This usually means the person has made threats, acted violently, or shown behavior suggesting others may be at serious risk.
- Grave disability: This means the person's psychiatric condition is affecting them so severely that they can't safely care for basic needs like food, clothing, or shelter.
These categories can sound cold on paper, but they show up in very human situations. A person with severe depression may stop eating and tell family they don't want to live. Someone in mania may become highly impulsive, paranoid, and unable to recognize obvious risks. A person in psychosis may wander, refuse care, or become so disorganized that they can't manage basic daily survival.
Practical rule: A 5150 is about immediate safety, not a final judgment about someone's character, future, or worth.
That distinction matters. Many patients feel ashamed after a hold. Many families feel guilty, angry, or split about whether calling for help was the right move. In a real crisis, the priority is keeping everyone alive and getting a clinical assessment.
Here's what often confuses families most:
| Situation | What people assume | What it usually means |
|---|---|---|
| A person was placed on a 5150 | “They'll now be in treatment long term” | The hold handles the emergency, not the whole recovery plan |
| A person is upset about being held | “The system is punishing them” | Distress is common even when the hold is for safety |
| A person looks calmer later | “The crisis is over” | Calm can be real, but ongoing support may still be needed |
If you're reading this right after a psychiatric emergency, the main thing to hold onto is simple. A 5150 is the crisis doorway. It's not the full road back.
Patient Rights During a 72-Hour Hold
What patients and families should expect
One of the hardest parts of a 5150 is the feeling that everything is happening to you or to someone you love, with no say at all. That's not how it's supposed to work. Even during an involuntary hold, patients still have rights, and families should know what respectful care looks like.
Patients should be told why they're being held. They should be informed that the hold is based on concerns about safety and that the facility is evaluating what level of care is appropriate next. Clear communication matters because confusion often increases fear, and fear can increase agitation.
Families can also help by asking calm, specific questions. What is the current plan. Who is the treating clinician. What are the rules around phone calls, updates, and discharge planning. Even when privacy limits what staff can share, respectful staff should still explain the general process.
Where confusion happens most often
Several rights and expectations tend to come up again and again:
- The right to be informed: Patients should receive information about the hold and the reason for it in language they can understand.
- The right to humane treatment: Safety precautions don't remove the obligation to treat someone with dignity.
- The right to ask about medications: Medication decisions can feel scary during a crisis. Patients and families often need plain-language explanations of what is being offered and why.
- The right to communication within facility rules: Phone access, visitor rules, and timing vary by setting, but patients can ask what is allowed.
- The right to legal process in the event of extended detention: If the hold goes beyond the initial emergency period, additional review matters.
Families often feel they need to either fight the staff or stay silent. Neither extreme helps. Calm advocacy usually works better.
It also helps to know what not to expect. You may not get immediate, full updates if privacy rules apply. You may not be able to visit the minute you want. The patient may also tell a very different story about what happened than the clinical team does. That mismatch is common in acute psychiatric crises.
A steadier approach is to focus on practical questions:
- What is the current safety concern
- What signs will show improvement
- What discharge options are being considered
- What support will be needed at home
- What level of care should come next if the person is released
When families understand those basics, the system feels less mysterious. It may still be painful, but it becomes easier to manage.
After 72 Hours Discharge and Extension Options
Three common paths after the hold
As the initial hold nears its end, most families ask the same question. What happens now? The answer usually falls into one of three paths.
The first possibility is release. If the treatment team believes the person is no longer meeting the emergency criteria, they may be discharged. That doesn't always mean the person is fully well. It means the immediate basis for involuntary emergency detention may no longer be present.
The second path is voluntary treatment. Sometimes a person agrees to stay for more care or agrees to enter a structured program after discharge. This can be a major turning point because treatment usually works better when the person participates willingly, even if they were resistant at the start.
The third path is an extension of care because the clinical team still believes the person remains unsafe or too impaired to leave.
What a 5250 means in simple terms
If you hear the term 5250, families often panic because it sounds like the crisis is getting bigger. In simple terms, it means clinicians believe the person still meets criteria for continued involuntary psychiatric treatment after the initial emergency period.
That doesn't mean the decision is supposed to happen in secret or without review. When an extension is pursued, the patient has a right to a legal review process connected to that continued hold. Families should ask staff to explain what stage the process is in and what the patient can expect next.
A simple way to think about the choices is this:
| End of initial hold | What it means for the patient | What the family should ask |
|---|---|---|
| Release | The emergency criteria may no longer be met | What outpatient support starts immediately |
| Voluntary stay | The person agrees to more treatment | What goals should be addressed before discharge |
| Extended hold | The team still sees serious safety concerns | What review process applies and what rights remain |
One point often gets missed. A person can leave a hold and still be very vulnerable. They may still have depression, panic, trauma symptoms, bipolar symptoms, psychosis-related recovery needs, substance use concerns, or major difficulty functioning at home. That's why discharge planning matters so much.
Leaving the hospital is not the same as being ready to manage life alone.
For many people, the safest next step isn't “go home and figure it out.” It's entering a structured voluntary program that picks up where crisis stabilization leaves off.
The Bridge to Recovery Partial Hospitalization Programs PHP
Why PHP is often called a day hospital
If inpatient care feels too restrictive, and weekly therapy feels far too light, Partial Hospitalization Programs often fill that gap. Many clinicians and families think of PHP as a day hospital. That description helps because it captures both parts of the experience. Treatment is intensive during the day, but the person returns home in the evening.
A mental health PHP typically involves 25 to 30 hours of structured programming per week, delivered Monday through Friday, and it serves as a step-down from inpatient treatment and a step-up from Intensive Outpatient Programs while allowing clients to return home (Renaissance Recovery on PHP in Orange County).
This comparison makes the differences easier to see.
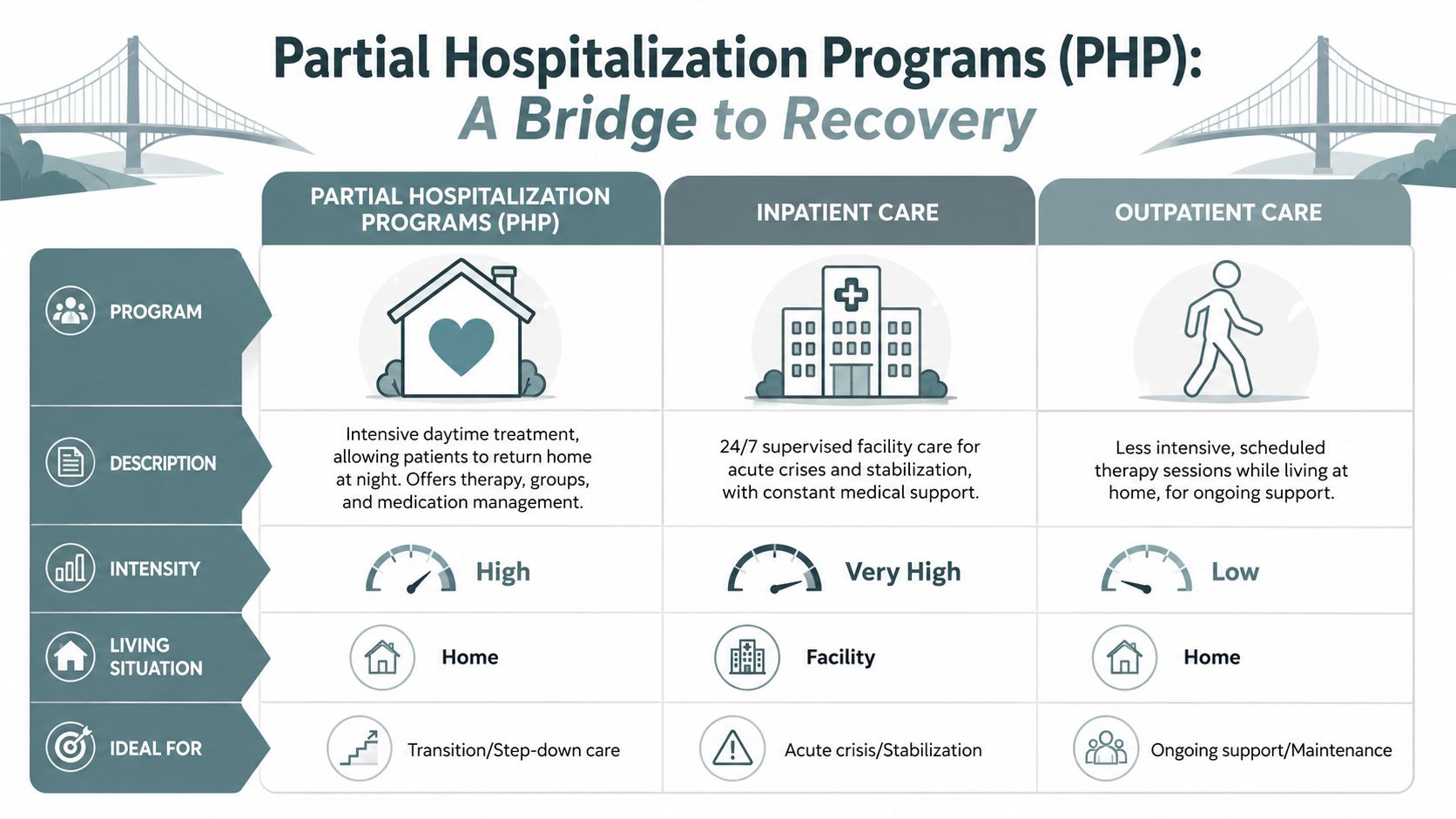
Someone stepping out of a psychiatric hold may need more than a single therapist visit every week. They may need daily therapy contact, medication support, a place to process the crisis, and structure strong enough to interrupt old patterns. PHP offers that middle ground.
What a PHP usually includes
Most families searching for PHP near me want to know what the days look like. A PHP is usually built around several forms of care working together:
- Individual therapy: Time to work on the personal story behind the crisis, not just the symptoms that brought someone into care.
- Group therapy: A structured setting where people practice coping skills, communication, and emotional regulation with support.
- Medication management: Psychiatric follow-up that helps monitor symptoms, side effects, and progress.
- Psychoeducation: Practical teaching about diagnoses, triggers, relapse warning signs, and daily functioning.
A useful way to compare levels of care is this:
| Level of care | Where the person lives | Support level |
|---|---|---|
| Inpatient | At a facility | Highest supervision during acute crisis |
| PHP | At home | High daytime structure and close oversight |
| Standard outpatient therapy | At home | Lower intensity, scheduled visits only |
For people trying to decide whether this level makes sense, a more detailed explanation of the benefits of a PHP program can help clarify what daily participation is meant to accomplish.
PHP often works best for people who are no longer in immediate need of round-the-clock hospitalization but still don't feel safe, steady, or functional enough for ordinary outpatient care. That's why it's such an important bridge after a 5150.
How PHP Prevents Re-Hospitalization and Builds Stability
Structure changes what happens between appointments
After a psychiatric crisis, the highest-risk time is often not the moment someone is sitting with a clinician. It's the long stretch between appointments. Hours at home can fill with panic, isolation, skipped medication, family conflict, substance use, poor sleep, or the return of hopeless thoughts. Weekly therapy rarely gives enough contact to catch those shifts early.
PHP changes that by creating repeated points of support through the week. In mental health care, PHPs provide 20 to 30 hours of structured clinical programming per week and can reduce symptom relapse by 35% compared to standard outpatient care, with the source attributing that benefit to continuous daily monitoring and rapid intervention (Casa Recovery on PHP in San Juan Capistrano).
That kind of structure matters because instability usually doesn't return all at once. People slide. They sleep less. They stop eating well. They miss medications. They withdraw. They start thinking in all-or-nothing terms. A program with daily contact can notice those patterns before they turn into another emergency.
Skills support and monitoring work together
PHP also works because it doesn't rely on insight alone. It gives people repeated practice. Someone with severe anxiety may learn grounding skills in the morning, try them that afternoon, and return the next day to talk through what happened. Someone with depression may set a simple behavioral goal, struggle with it, and get immediate help adjusting the plan instead of waiting another week.
Three parts of PHP tend to reinforce each other:
Daily routine
Crisis disrupts sleep, meals, hygiene, movement, and time awareness. A set treatment schedule starts rebuilding those basics.Close clinical contact
Problems can be addressed quickly. A rise in symptoms doesn't have to become a full relapse before anyone notices.Peer environment
Many people leave a hold feeling ashamed or alone. Sitting with others who also understand psychiatric distress can reduce that isolation.
If you're weighing PHP against a lower level of care, this overview of PHP vs IOP for mental health can help you think through which setting matches the person's current level of instability.
Recovery after a 5150 usually isn't about one breakthrough conversation. It's about enough support, often enough, for long enough, that the person can function safely outside the hospital.
PHP can't remove every setback. No program can. But it gives people a stronger chance to stabilize before stress, symptoms, or confusion push them back into crisis care.
Finding Hope and Healing at Casa Recovery
What makes this level of support useful after a crisis
For adults in Orange County who need structured outpatient mental health care, Casa Recovery offers PHP as one of the highest levels of outpatient support available. Their PHP provides daily clinical oversight for conditions including depression, anxiety, trauma, and co-occurring disorders, with an average duration of 4 to 8 weeks adjusted based on individual progress (Casa Recovery PHP program details).
That time frame can help families who are scared that treatment will either end too fast or go on without direction. A program measured in weeks, with care adjusted to progress, gives room for stabilization while keeping the focus on forward movement.
Here is the program page many families review when comparing options.
Who may benefit most
Some people need a setting that can address more than one problem at a time. That includes adults dealing with trauma plus depression, anxiety plus substance use, or mood instability plus family stress. Casa Recovery's model is designed around evidence-based outpatient treatment, dual-diagnosis care, onsite psychiatry, and a strong trauma-informed focus.
A few features stand out for people leaving a hospital or hold:
- Small groups and personalized attention: This can matter when someone feels flooded, distrustful, or easily overwhelmed.
- Integrated psychiatric care: Medication support and psychotherapy happen within one coordinated outpatient setting.
- Dual-diagnosis treatment: Mental health symptoms and substance use concerns can be addressed together instead of split apart.
- Family involvement: Education and communication with families can reduce confusion at home.
What many families need after a crisis isn't a generic referral list. They need a place where the person can keep working on symptoms, daily functioning, and safety without dropping abruptly from hospital-level concern to almost no structure at all. That's the gap PHP is meant to fill.
Your Immediate Next Steps to Getting Help
A simple action plan for families in Orange County
When everything feels urgent, a short plan helps. Don't try to solve the next six months tonight. Focus on the next right steps.
Ask for the discharge plan in writing
If your loved one is still in a facility, ask what level of care the team recommends next. If they mention PHP, ask why that level fits better than standard outpatient therapy or IOP.Call a program and describe the crisis clearly
Don't minimize what happened. Say if there was a 5150, suicidal thinking, psychosis, substance use, or severe functional decline. That helps the admissions team judge whether PHP is appropriate.Verify insurance and timing quickly
Good programs can help check benefits and discuss admission logistics. Delays after discharge can leave people unsupported at the exact moment they need structure.Schedule an assessment
A clinical assessment helps determine whether PHP is the right fit now or whether another level of care makes more sense. If you need a starting point, Casa Recovery explains how to take the steps to admit yourself to mental health treatment.Prepare the home environment
Remove obvious safety risks if clinicians recommend it. Simplify responsibilities. Plan transportation. Decide who will handle medication pickup, meals, and check-ins.Use trustworthy educational resources while you decide
Families often search online in a panic and end up buried in marketing. If you want a broader example of how healthcare organizations try to improve local visibility and patient access online, this guide to patient acquisition strategies for medical clinics can help you understand why some programs appear first in search results and why it's worth reading carefully before choosing.
One last point matters. If your loved one is actively unsafe right now, don't wait for a PHP intake call. Use emergency services or return to the nearest emergency department. PHP is a strong next step after immediate danger is addressed. It isn't a substitute for emergency intervention during an active crisis.
Recovery usually starts messily. People may feel embarrassed, skeptical, tired, or angry. Families may feel burned out. None of that means treatment won't work. It means you're in the hard middle, and the hard middle is exactly where structured support can help.
If you or someone you love needs a clear path forward after a psychiatric crisis, Casa Recovery can help you explore whether PHP or another outpatient level of care is the right next step. A confidential conversation with their team can help you understand treatment options, insurance, and how to move from crisis toward real stability.