When mental health symptoms start affecting work, sleep, relationships, or basic daily life, many people do the same thing first. They search late at night, read a few provider pages, and end up more overwhelmed than when they started. The words sound clinical. The options blur together. You may be wondering what happens once treatment begins, who decides what care looks like, and whether there's a real plan or just a series of appointments.
That uncertainty is hard on families too. A spouse may want to help but not know what to say. A parent may hear terms like PHP, IOP, CBT, DBT, or EMDR and feel like everyone else got a handbook they never received. When people are scared, they often assume treatment planning is just paperwork. In practice, a good plan does something much more important. It gives structure to recovery.
A mental health treatment plan is best understood as a roadmap. It helps you answer practical questions: What are we treating? What are the goals? Which therapies fit those goals? How will progress be measured? What happens if the first approach needs adjustment? Research supports the value of this kind of planning. When a clinical target is included in a treatment plan, the odds of it being addressed are 3.10 times higher, and practices listed in the plan are over two times more likely to be implemented, according to findings published in this treatment planning study.
For some families, access starts with communication. If a client or loved one is Deaf or hard of hearing, arranging professional ASL interpreting can make assessments, family meetings, and consent discussions much clearer and more respectful.
Table of Contents
- Your Roadmap to Recovery An Introduction
- The Building Blocks of an Effective Treatment Plan
- Tailoring Your Plan for PHP IOP and Dual Diagnosis
- Integrating Specialized Therapies and Family Support
- What a Treatment Plan Looks Like in Action
- Navigating Insurance Admissions and Next Steps
Your Roadmap to Recovery An Introduction
People usually arrive at treatment planning mentally exhausted. They've often spent weeks trying to hold everything together while symptoms grow louder. Some are dealing with panic, depression, trauma reactions, mood swings, or substance use alongside emotional distress. Others are watching someone they love struggle and trying not to make things worse.
A strong plan can reduce that fear because it replaces guesswork with direction. Instead of asking, “What's wrong with me?” or “Where do we even begin?” the conversation shifts to something more useful. What patterns are showing up? What diagnosis fits the full picture? What needs the most support right now?
A good treatment plan isn't a judgment. It's a working map that helps a team respond to what's actually happening in your life.
In treatment planning mental health care, the most helpful plans are collaborative. They don't just list symptoms. They connect symptoms to goals, interventions, time frames, and ways to measure whether care is helping. That gives clients and families something solid to hold onto.
You should be able to understand your plan in plain language. If a goal says “improve emotional regulation,” a good clinician should translate that into real life. It may mean fewer explosive arguments, less self-isolation, more consistent sleep, or using coping skills before a crisis escalates. The point isn't to sound impressive. The point is to make care usable.
The Building Blocks of an Effective Treatment Plan
A treatment plan gives treatment structure. It turns a long list of worries, symptoms, and unanswered questions into a working clinical process that the client, family, and treatment team can follow.
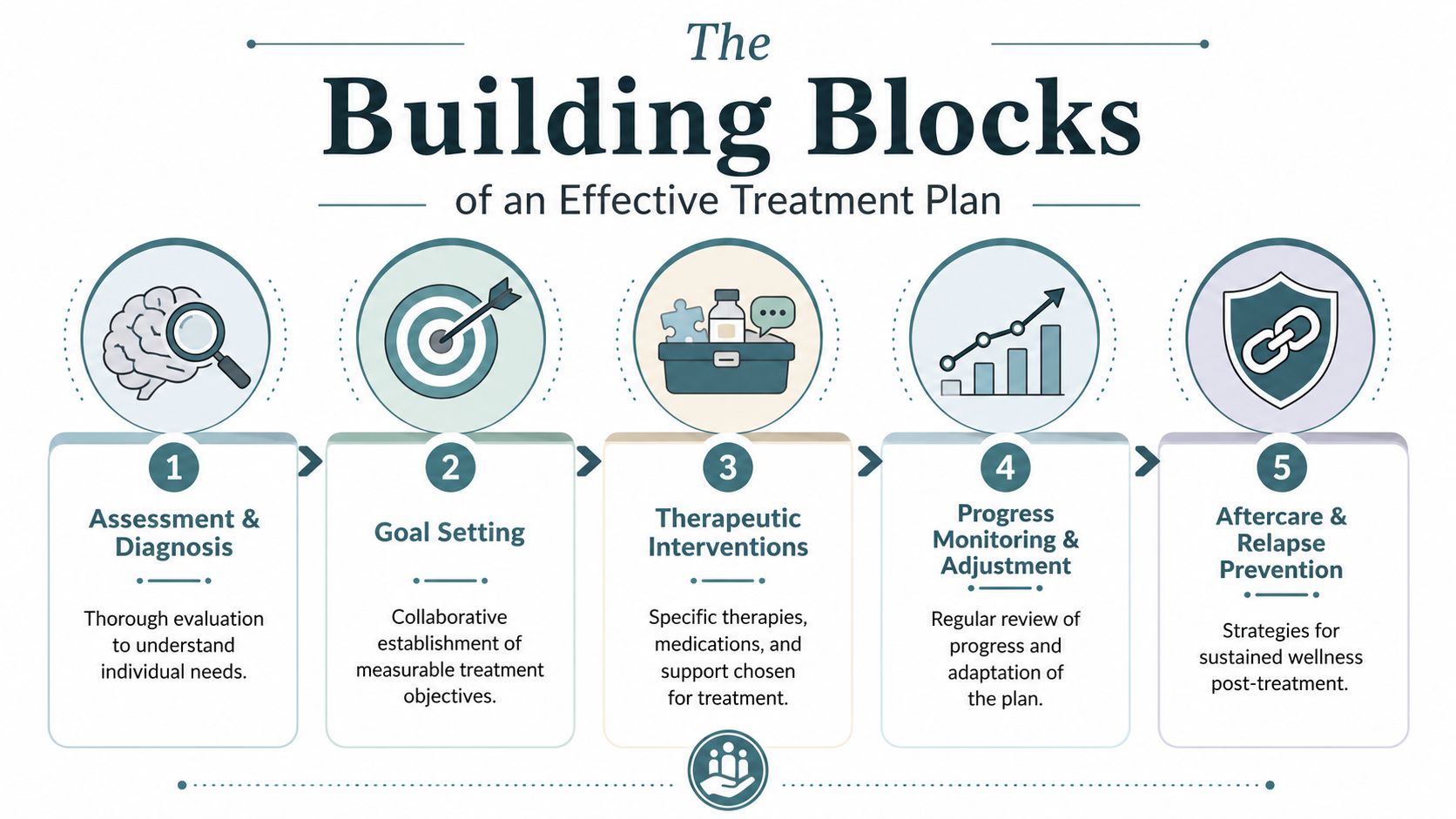
At a high-quality outpatient program, the plan is built in layers. The first layer answers, "What is happening right now?" The next asks, "What needs to change first?" Then the team decides, "Which therapies, supports, and level of care fit this person's real life?"
Assessment and diagnosis come first
The starting point is a careful assessment. That means more than listing symptoms on an intake form. A clinician looks at current distress, psychiatric history, trauma exposure, medical concerns, substance use, sleep, family relationships, risk factors, strengths, and how daily functioning has changed. If someone cannot get through work, is isolating at home, or is using substances to manage panic, those details shape the plan.
This early stage often brings relief. Families are no longer guessing whether they are looking at anxiety alone, trauma responses, depression, bipolar symptoms, substance use, or several issues interacting at the same time.
Diagnosis helps organize care. In a strong outpatient setting such as Casa Recovery, the diagnosis is connected to what the client is experiencing day to day, not treated like a label that defines them. If the team identifies both mental health symptoms and substance use, the plan should address both from the start. If trauma is part of the picture, that affects pacing, safety planning, and the choice of therapies later on.
Here is the difference between vague planning and usable planning:
| Clinical area | Vague version | Useful version |
|---|---|---|
| Anxiety | Feel less anxious | Practice grounding during panic symptoms and return to the task at hand |
| Depression | Improve mood | Rebuild a daily routine, increase activity, and reduce time spent isolated |
| Emotional regulation | Control emotions | Use distress tolerance skills during conflict and review what worked in therapy |
Goals should be specific enough to guide care
A good goal should make sense in plain language. Clients should be able to read it and know what they are working on this week, not just what the chart says in general terms.
That is where many plans either become too broad or too technical. "Improve emotional regulation" may be clinically accurate, but it still needs translation. Does that mean fewer angry outbursts, less shutting down, more stable sleep, or asking for support before a crisis builds? The answer matters because treatment becomes more effective when the goal connects to real behavior.
Clear goals usually answer four practical questions:
- What is changing: panic symptoms, trauma triggers, cravings, depressed mood, impulsive behavior, or conflict at home
- What the client will practice: CBT skills, DBT coping tools, relapse prevention strategies, journaling, exposure work, or communication skills
- Where the problem shows up: home, work, school, relationships, or recovery environments
- How the team will know it is helping: self-report, therapist observation, symptom measures, attendance, and daily functioning
Families often find this easier to understand when they see goals translated into everyday progress. This explanation of setting meaningful goals during recovery gives a clear example of what that can look like outside clinical language.
A simple test helps here. If the client cannot explain the goal back in their own words, the goal needs to be rewritten.
Interventions roles and review keep the plan active
Once the goals are clear, the team chooses interventions that match the problem and the client's current stability. This is the operational part of treatment planning that people often do not get to see.
For one person, that may mean individual therapy, group therapy, medication management, and coping-skills practice several days a week. For another, it may mean starting with stabilization work before trauma processing begins. A client with both substance use and depression should not receive two disconnected plans. The care should be integrated so relapse prevention, mood treatment, and psychiatric support all pull in the same direction.
Roles also need to be clear. The primary therapist tracks progress and updates goals. The psychiatrist evaluates symptoms, medications, and safety. Group clinicians reinforce skills in real time. The client practices those skills between sessions. Family members may be invited into the process so they know how to support recovery without stepping into constant crisis management.
Review matters because treatment is a living process. Clinicians regularly check whether symptoms are easing, whether attendance and functioning are improving, and whether the current approach still fits. Sometimes the plan stays steady. Sometimes it needs adjustment because trauma symptoms become more visible, substance use risk increases, or the client is ready for more focused work such as EMDR after a stronger foundation has been built.
A good plan does not sit in a chart untouched. It is updated, discussed, and used. That is what helps outpatient care feel organized, responsive, and realistic for the person living it.
Tailoring Your Plan for PHP IOP and Dual Diagnosis
Not every outpatient plan should look the same. Someone who needs daily structure, close monitoring, and frequent therapeutic contact needs a very different plan from someone who is stable enough to work, attend school, or care for family while receiving treatment several times a week.
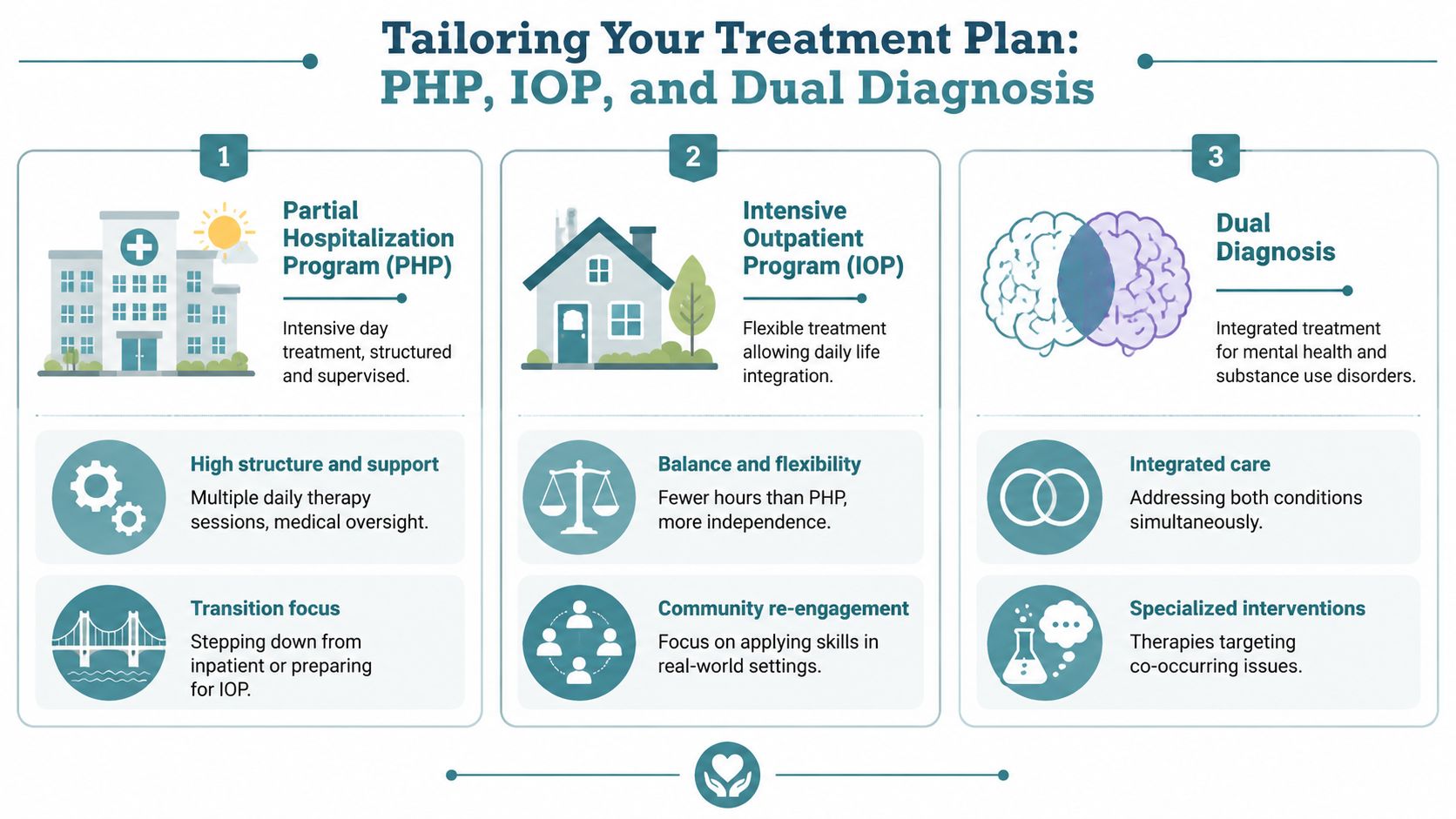
How PHP and IOP plans differ in daily life
A Partial Hospitalization Program (PHP) plan is usually more structured. The client may need strong containment around mood instability, trauma symptoms, severe anxiety, early recovery, or recent decompensation. In PHP, treatment planning often emphasizes daily therapeutic engagement, rapid feedback, medication coordination, and frequent support with coping skills before symptoms spiral.
An Intensive Outpatient Program (IOP) plan usually has a different rhythm. The work often focuses on practicing recovery in everyday life while staying connected to meaningful clinical support. A client in IOP may be rebuilding routines, navigating work stress, managing family roles, or learning how to use new coping skills outside the treatment setting.
This comparison helps clarify the difference:
| Level of care | Treatment plan emphasis | Common operational focus |
|---|---|---|
| PHP | Stabilization and structure | Frequent monitoring, intensive therapy, close coordination |
| IOP | Reintegration and consistency | Applying skills at home, work, school, and relationships |
A generic plan misses these practical differences. A personalized one accounts for how much support a person needs, what their current environment is asking of them, and how quickly the team needs to assess response.
Why dual diagnosis needs one unified plan
Dual diagnosis planning is where many systems fall short. A person may have depression, trauma, bipolar symptoms, or anxiety while also struggling with alcohol or drug use. Treating one problem first and the other later often creates fragmentation. The person ends up carrying the burden of coordinating care while already overwhelmed.
That approach doesn't fit what we know about co-occurring disorders. Fifty percent of individuals with substance use disorders also have a mental health condition, and evidence reviewed in this dual-diagnosis publication shows that integrated models treating both conditions within one plan improve continuity of care and reduce relapse.
When mental health symptoms and substance use feed each other, the treatment plan should address both in the same conversation, with the same goals, and through one coordinated team response.
In operational terms, that means the plan might include trauma work, relapse prevention, psychiatric review, coping skills for cravings, sleep stabilization, and family boundaries all at once. Not because the plan is trying to do everything, but because real life doesn't separate problems as neatly as some programs do.
Integrating Specialized Therapies and Family Support
Specialized therapies should never feel random to a client. If a plan includes EMDR, Brainspotting, psychiatry, or family therapy, each piece should have a clear reason tied to the assessment, the diagnosis, and the current treatment goals.

Trauma therapies are chosen for a reason
When trauma is part of the clinical picture, the plan often needs more than supportive talk therapy. A client may understand intellectually why they react strongly, yet still feel hijacked by body-based fear, flashbacks, hypervigilance, shame, or shutdown. That's where trauma-focused therapies can serve a specific role.
EMDR is often integrated when trauma memories remain highly activating and the client has enough stability to process them safely. Brainspotting may be considered when trauma feels stuck in a way that's difficult to verbalize. These therapies are not stand-alone fixes. They usually sit inside a broader plan that also includes grounding, distress tolerance, sleep support, emotional regulation, and pacing.
Some clients need preparation before trauma processing begins. Others need longer stabilization because pushing too quickly can backfire. A thoughtful plan respects that timing.
Psychiatry and family work strengthen the core plan
Psychiatric care is another area families often misunderstand. Medication management isn't separate from therapy. In a well-run outpatient program, it's a coordinated part of the same plan. If severe depression, panic, insomnia, mood instability, or intrusive trauma symptoms are limiting a client's ability to engage, psychiatric support may help create the stability needed for therapy to work better.
Evidence-based protocols reduce distress, and the strongest outcomes are often seen when psychosocial interventions such as CBT are combined with psychopharmacology such as SSRIs, according to this review on goal-directed evidence-based treatment protocols. The key phrase is combined thoughtfully. Medication should support the work, not replace it.
Family involvement can be just as important. Symptoms don't happen in a vacuum. They affect communication, trust, routines, crisis response, and expectations at home. When families are included appropriately, the treatment plan can target specific relational goals such as reducing enabling, improving boundaries, increasing supportive communication, and helping loved ones respond more effectively during difficult moments.
For many families, structured education and therapy make the process less confusing. This resource on the benefits of family therapy gives a useful overview of why family participation often improves the treatment environment.
- Trauma therapy fits a target: It's chosen when trauma symptoms are central to current impairment.
- Psychiatry supports stabilization: It can reduce barriers that prevent effective participation in therapy.
- Family work changes the environment: It helps recovery continue outside the therapy room.
What a Treatment Plan Looks Like in Action
A good treatment plan becomes easier to understand when you can see how it works in daily life. Families often expect a generic checklist. What they receive in a strong outpatient program is closer to a working schedule with clinical priorities, clear responsibilities, and regular course correction.
At Casa Recovery, the plan is built to answer practical questions. How many treatment hours does this person need each week? What symptoms are getting in the way of daily life right now? What has to stabilize first so deeper therapy can be useful? Which parts of the plan belong in group work, which belong in individual therapy, and where should psychiatry or family sessions fit?
Vignette one anxiety and depression in IOP
Sarah is a young adult whose anxiety fills most of the day. She is still meeting some responsibilities, but at a high cost. She avoids calls, misses deadlines, cries alone, and stays awake replaying conversations long after they end.
Her team recommends IOP because she needs more structure than weekly therapy can offer, while still being able to live at home and practice new skills between sessions. That schedule matters. It gives her repeated contact each week, enough support to interrupt the cycle, and enough real-world exposure to see what is and is not working.
Her treatment plan is organized in layers. Group sessions focus on CBT skills for anxious thinking, avoidance, and depressive shutdown. Individual therapy targets perfectionism, shame, and the specific situations that trigger spiraling. Case coordination tracks sleep, work demands, and follow-through on daily tasks. If symptoms block participation, psychiatric review can be added to help reduce that barrier.
The goals are concrete and measurable: restore a sleep routine, reduce avoidance, answer missed communications, and return to responsibilities in smaller, manageable steps. Treatment works like a flight plan. The destination is important, but the team also keeps checking direction, weather, and altitude so small problems do not turn into a larger setback.
Vignette two PTSD and alcohol misuse in PHP
Mark enters PHP after trauma symptoms and alcohol misuse begin reinforcing each other. He has nightmares, irritability, emotional numbing, and a pattern of drinking at night to get through the distress. A weekly appointment would leave too much time between points of contact. He needs a higher level of outpatient structure, more observation, and faster adjustment when symptoms change.
His plan does not split mental health treatment from substance use treatment. It addresses both at the same time, because each problem affects the other. The daily PHP framework includes group therapy, individual sessions, psychiatric support, relapse prevention work, and close monitoring of sleep, triggers, cravings, and trauma activation.
Timing matters here. Early treatment may focus first on safety, stabilization, and distress tolerance. Once Mark can stay present without becoming overwhelmed, the team can begin trauma-focused work more directly. If EMDR is clinically appropriate, it is added carefully, not rushed, and only when he has enough grounding skills to use it well.
Family participation can also be scheduled into the plan. Loved ones may learn how trauma symptoms show up at home, how substance use changes communication, what responses reduce escalation, and what boundaries support recovery instead of rescuing the pattern. That turns family sessions into part of the operating plan, not a side conversation.
For families trying to picture how goals, interventions, and follow-up fit together, it can help to understand your medical care plans through examples outside behavioral health as well.
Plans like these are living documents. The team reviews attendance, symptom patterns, functional changes, setbacks, and treatment response, then adjusts frequency, goals, or modalities as needed. If you are preparing for care and want to clarify coverage before those decisions are made, you can verify insurance for outpatient mental health treatment early.
Navigating Insurance Admissions and Next Steps
Starting care often feels hardest before treatment even begins. People worry about insurance, privacy, paperwork, travel, and whether they'll be told they need a level of care they don't understand. Clear admissions processes reduce that friction.

From the first call to the clinical recommendation
The process usually begins with a phone call. The admissions team gathers basic concerns, current symptoms, safety issues, prior treatment history, and insurance information. This first step isn't the full clinical assessment, but it helps determine urgency and whether the program may be a fit.
Insurance verification comes next. Families often hear terms like PPO, in network, out of network, deductible, or authorization and feel lost. A good admissions team explains what benefits may apply and what questions still need clarification. If you're exploring options, verify insurance for behavioral health treatment early so you're not trying to sort out coverage in the middle of a crisis.
Then, the pre-admissions assessment involves clinicians evaluating symptoms, diagnosis, functional impairment, substance use if relevant, medical and psychiatric needs, and the most appropriate level of care. The recommendation should match the client's clinical presentation, not just convenience.
A typical sequence looks like this:
- Initial inquiry: Share what's happening now and what kind of support you're seeking.
- Benefits check: Review insurance details and any financial questions.
- Clinical assessment: Determine safety, diagnostic picture, and level of care.
- Admissions paperwork: Complete consent forms, history, and program documents.
- Orientation and intake: Meet the team, review the schedule, and begin treatment.
Insurance privacy and transitions of care
Privacy matters throughout admissions and treatment. When records, assessments, and care coordination are handled electronically, families often want reassurance that sensitive health information is protected. A plain-language guide to understanding HIPAA compliance rules can help clients know what secure handling of health information should look like.
For people coming from outside the area, supportive living may also be part of the planning conversation. The goal is practical stability. A safe place to stay, reliable transportation, and consistent routines can make it much easier to engage in PHP or IOP.
Discharge planning starts earlier than many people expect. A strong outpatient plan includes transitions of care from the beginning. That might mean stepping down from PHP to IOP, moving to less frequent therapy, continuing psychiatry, joining alumni or recovery supports, or building a family follow-up plan. Recovery is stronger when people don't leave treatment with no bridge to the next phase.
If you're looking for structured, trauma-informed outpatient mental health or dual-diagnosis care in Southern California, Casa Recovery offers PHP, IOP, psychiatry, family programming, and specialized therapies designed to fit real-world recovery. Reaching out for an assessment can turn a stressful unknown into a clear next step.