You may be reading this after a diagnosis, after a panic-filled night, or after years of trying to explain symptoms that never seemed to make sense to other people. Maybe you're the one with PTSD. Maybe you're the spouse, parent, or adult child trying to help and not make things worse. Either way, the same question usually shows up fast: what exactly are we trying to accomplish in treatment?
That question matters because trauma treatment can feel confusing at first. One clinician talks about grounding. Another recommends EMDR. Someone else mentions medication, sleep, group therapy, or a higher level of care. When you're already exhausted, that can sound like a pile of disconnected ideas instead of a plan.
A good treatment plan isn't random. It gives recovery direction. In plain terms, post traumatic stress disorder treatment goals are the practical targets that help a person move from surviving the day to living with more safety, stability, connection, and freedom.
Table of Contents
- Navigating Recovery After a PTSD Diagnosis
- What Are PTSD Treatment Goals Really
- The Five Pillars of PTSD Recovery Goals
- Creating SMART Goals for PTSD Treatment
- How Therapies Like EMDR and CBT Achieve Your Goals
- Goal-Oriented Treatment at Casa Recovery
- Frequently Asked Questions About PTSD Treatment Goals
Navigating Recovery After a PTSD Diagnosis
A new PTSD diagnosis often lands with two opposite feelings at once. There's relief because the symptoms finally have a name. There's also fear because the name sounds heavy, and people worry it means life will never feel normal again.
I often think of early treatment like getting handed a map after being lost in the dark. The map doesn't erase what happened. It doesn't force you to sprint. It shows where you are, what needs attention first, and what direction leads toward steadier ground.
For one person, the first urgent problem may be sleep. For another, it's panic while driving, rage at home, or shutting down in relationships. A family may notice isolation, irritability, drinking, or emotional numbness long before they understand those behaviors as trauma responses. That's why treatment goals need to be personal. The right plan doesn't treat a diagnosis in the abstract. It treats the way PTSD is affecting this person's body, mind, routine, and relationships.
Recovery usually starts with one calming idea: you do not have to fix everything at once.
The most helpful goals are not rigid orders. They are signposts. They help answer questions like:
- What needs attention first: safety, sleep, flashbacks, substance use, or daily functioning
- What progress would look like: fewer shutdowns, better work attendance, less avoidance, or stronger relationships
- What support fits best right now: outpatient therapy, intensive outpatient care, or a partial hospitalization program
When people understand their goals, treatment becomes less mysterious. It starts to feel like a coordinated process instead of a series of emotional experiments. That shift matters. Hope grows when recovery becomes concrete.
What Are PTSD Treatment Goals Really
Many people assume PTSD treatment goals mean one thing: make the symptoms stop. That is part of the work, but it's not the whole picture. If we only focus on flashbacks, nightmares, or anxiety spikes, we can miss the larger question. How do you build a life that feels livable again?
A better way to think about treatment is to imagine rebuilding a damaged home. Symptom reduction is like stopping the roof from leaking. It's necessary. But a repaired roof alone doesn't make the home warm, safe, connected, and useful. Recovery also includes restoring daily routines, trust, purpose, and relationships.
A recent veteran study found that patients prioritize symptom improvement, personal well-being or growth, and restoration of social roles and interpersonal functioning, while standard templates often lean heavily toward symptom metrics, as described in this 2024 veteran-centered study. That gap explains why some people say, “My symptoms are a little better, but I still don't feel like myself.”
Recovery includes more than symptom counts
Clinically, goals often include emotional regulation, coping skills, and trauma processing. In real life, people usually talk about different things. They want to sleep through the night, stop snapping at their kids, go to the grocery store without scanning for danger, feel close to a partner again, or stop avoiding memories that hijack the whole day.
Those are not “soft” goals. They are central goals.
Here's what families often find confusing. A trauma therapist may celebrate progress that looks small from the outside. Someone sits with a difficult feeling without leaving session. Someone uses a grounding skill before dissociating. Someone drives past a trigger instead of turning around. These are not minor wins. They are the early signs that the nervous system is becoming more flexible and less trapped in survival mode.
The real target is a fuller life
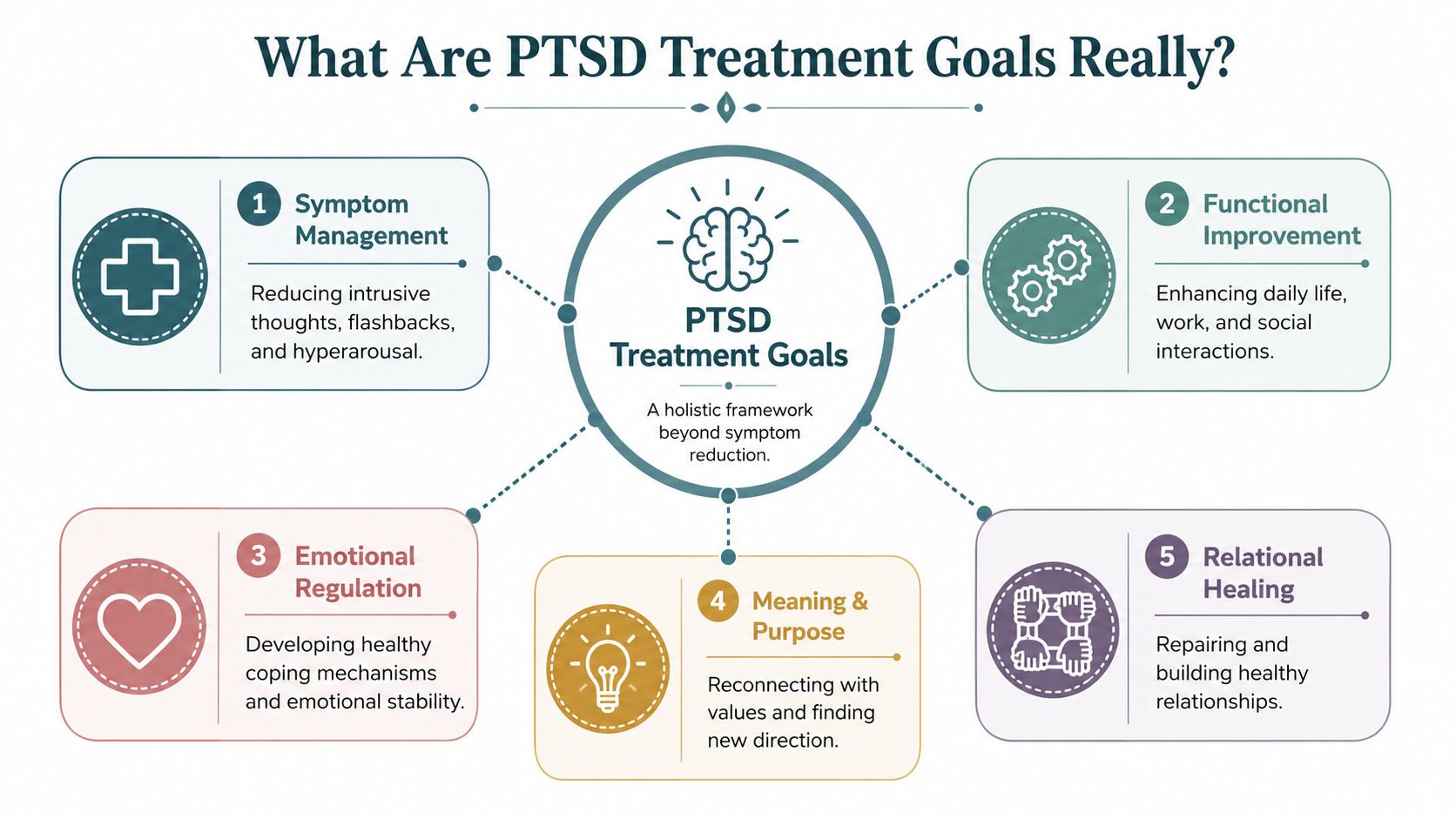
A strong PTSD plan usually addresses several layers at once:
- Symptom management: reducing intrusive memories, hyperarousal, avoidance, and sleep disruption
- Functional improvement: helping the person work, parent, study, socialize, and care for themselves more consistently
- Emotional healing: increasing tolerance for difficult feelings without shutting down, exploding, or numbing out
- Meaning and identity: reconnecting with values, strengths, and a sense of self beyond the trauma
- Relational repair: rebuilding trust, communication, and safe connection with other people
The goal is not to become the person you were before trauma. The goal is to help you live more freely now.
That mindset changes treatment. It keeps therapy from becoming a checklist and turns it into a practical roadmap for recovery.
The Five Pillars of PTSD Recovery Goals
Some treatment plans look complicated because they contain many moving parts. In practice, most post traumatic stress disorder treatment goals fit into five broad pillars. Thinking this way helps people see the whole plan without getting lost in the details.
Symptom relief is only the starting point
This is the pillar widely expected. It includes reducing flashbacks, nightmares, intrusive thoughts, panic reactions, hypervigilance, and avoidance. These symptoms drain energy and make everyday life feel unsafe.
Recent clinical framing has shifted toward functional recovery, not just symptom elimination, and trauma-focused psychotherapy is recommended in 12 to 16 weekly sessions in the guideline summary cited by The Recovery Village. That same summary reports that treated individuals have symptoms for an average of 36 months, compared with 64 months for untreated individuals. That difference matters because it shows why early, structured care is worth pursuing.
Function matters as much as distress
A person can have fewer symptoms and still struggle to live well. Functional goals ask different questions. Can you get out of bed on time? Keep appointments? Drive, work, attend school, or manage parenting demands with less chaos? Can you tolerate ordinary stress without feeling hijacked?
Functional recovery often sounds ordinary. That's exactly why it matters. Ordinary life is what trauma often steals.
Examples include:
- Daily routine: waking, eating, and sleeping on a steadier schedule
- Role performance: returning to work tasks, school demands, or caregiving responsibilities
- Community life: shopping, attending appointments, or being in public with less fear and avoidance
Safety has to be built on purpose
Trauma can create a constant sense of danger, even when no immediate threat is present. Good treatment goals include a clear safety plan for emotional flooding, self-harm risk, relapse risk, or crisis situations. Safety goals also include learning how to notice early warning signs before things spiral.
This pillar often starts with basic nervous system skills. Breathing, grounding, distress tolerance, body awareness, and limits around overwhelming triggers are not side tasks. They are part of the core work.
Practical rule: if a person cannot stay present enough to benefit from trauma work, stabilization becomes the immediate goal.
Co-occurring issues need their own goals
PTSD rarely travels alone. Depression, anxiety, substance use, dissociation, grief, and sleep disturbance can all complicate treatment. When these issues are ignored, progress often stalls because the person is fighting on too many fronts at once.
That's why a good plan doesn't say, “Let's handle the trauma first and everything else later.” It sets parallel goals that support each other.
Relationships are part of recovery
Trauma changes how people connect. Some become distant. Some become reactive. Some feel guilty, ashamed, or emotionally unreachable. Family members often misread these changes as lack of effort or lack of love.
Relational goals bring recovery back into everyday life. They may involve honesty, boundaries, communication, conflict repair, or reconnecting with healthy support. For many people, healing starts to feel real when home becomes calmer and relationships become safer.
Creating SMART Goals for PTSD Treatment
Vague goals create vague treatment. “Feel better” is understandable, but it's too broad to guide care. PTSD treatment works better when hopes are translated into concrete steps that both the client and treatment team can track.
That is where SMART goals help. SMART means Specific, Measurable, Achievable, Relevant, and Time-bound. Instead of saying, “I want less anxiety,” a SMART version might focus on one behavior, one setting, and one time frame.
What SMART goals look like in trauma care
The most useful trauma goals are small enough to practice and meaningful enough to matter. They should match the person's current level of care. Someone in a partial hospitalization program may need immediate stabilization goals. Someone in weekly outpatient therapy may focus more on maintaining gains and processing patterns over time.
Validated tools help keep this process grounded. Effective treatment plans commonly use the PCL-5, PHQ-9, and GAD-7 to monitor progress, and SMART goals may include targets such as reducing sleep latency to 30 minutes or less on at least 5 nights per week by week 10, as described in this guidance on PTSD treatment planning and measurement.
For readers who want a broader overview of how clinicians organize measurable psychiatric goals, this guide to mental health treatment planning is a useful reference.
SMART PTSD Treatment Goal Examples by Level of Care
| Goal Pillar | Partial Hospitalization (PHP) Goal Example | Intensive Outpatient (IOP) Goal Example | Outpatient Therapy Goal Example |
|---|---|---|---|
| Symptom management | Client will demonstrate 2 grounding skills in group and individual sessions when trauma cues trigger dissociation within the next 2 weeks | Client will identify early signs of flashback escalation and use a coping plan during at least 3 trigger situations over the next month | Client will track nightmare frequency weekly and practice a bedtime regulation routine consistently between sessions |
| Functional recovery | Client will attend scheduled programming consistently and complete a morning routine before arrival during current level of care | Client will resume one meaningful responsibility, such as work preparation or household tasks, on a predictable weekly schedule | Client will increase participation in one avoided daily activity, such as driving, shopping, or social contact, with therapist support |
| Emotional regulation | Client will name emotions and body sensations in session instead of shutting down when distressed | Client will use DBT-style distress tolerance skills before reacting impulsively in at least 2 real-life conflicts | Client will practice identifying trauma-linked beliefs and replace one unhelpful thought pattern each week |
| Safety and relapse prevention | Client will complete a written safety plan and rehearse who to call, where to go, and what coping steps to use during crisis states | Client will recognize personal relapse triggers and review the plan with the treatment team and family support | Client will maintain a personalized coping and support plan for high-stress periods and review it in therapy regularly |
| Family and social reintegration | Client will participate in family sessions and identify 2 communication needs during treatment | Client will practice one boundary-setting or repair conversation with support from the therapist | Client will strengthen one safe relationship through scheduled check-ins and improved communication patterns |
A strong SMART goal should answer three questions quickly:
- What exactly will change
- How will we know it is changing
- By when should we review it
That structure lowers confusion. It also reduces shame. People can see progress in pieces instead of feeling like they've failed because they aren't “all better” yet.
How Therapies Like EMDR and CBT Achieve Your Goals
Once goals are clear, the next question is practical. How does therapy help a person reach them?
Different therapies do different jobs. None of them are magic. Each one is a method for targeting a specific part of the trauma response.
How first-line trauma therapies work
The 2023 VA/DoD Clinical Practice Guideline recommends individual, manualized trauma-focused psychotherapies such as Prolonged Exposure (PE), Cognitive Processing Therapy (CPT), and EMDR as first-line interventions, delivered in 12 to 16 weekly sessions, as outlined in the VA overview of trauma-focused psychotherapy.
That matters because treatment goals should match the therapy's mechanism:
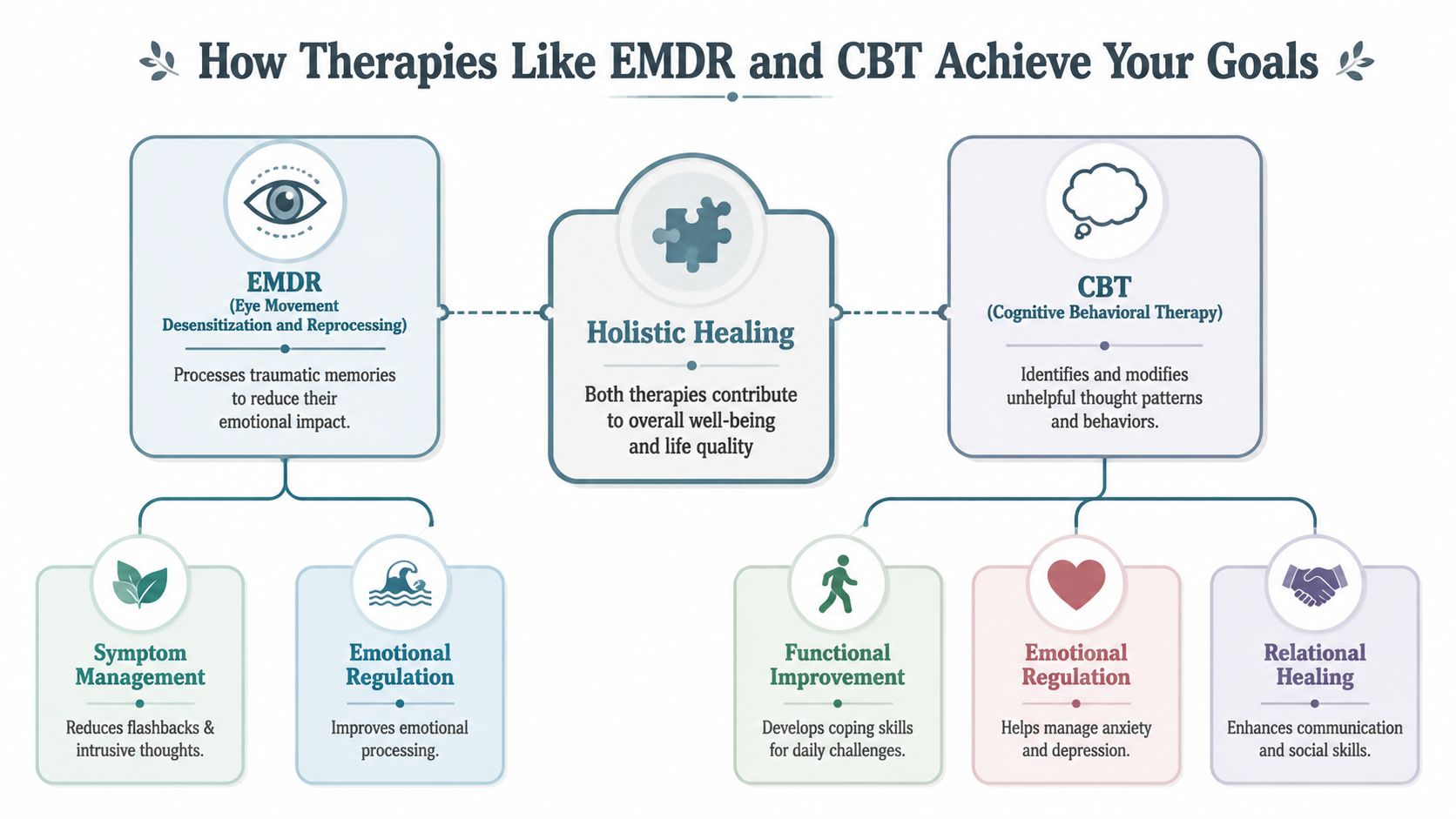
- EMDR: often helps reduce the emotional charge attached to traumatic memories. A client may still remember what happened, but the memory can become less overwhelming and less disruptive.
- CPT: focuses on trauma-related beliefs. It helps people examine stuck points around safety, trust, guilt, control, or self-worth.
- PE: helps reduce fear and avoidance through gradual, supported exposure to memories and situations that have remained linked to danger.
If you're trying to understand one of these approaches more clearly, this overview of EMDR therapy breaks down how that method is commonly used in trauma treatment.
How supportive therapies help between trauma sessions
Not every goal requires direct trauma processing right away. Some goals are about building the capacity to do that work safely.
CBT can help people notice patterns such as catastrophizing, self-blame, or rigid danger scanning. DBT skills can improve distress tolerance, emotional regulation, and interpersonal effectiveness. Group therapy can reduce shame by helping people experience that trauma responses are understandable, not bizarre.
Telehealth also changes access for many clients, especially those balancing care with work, family, transportation, or health limitations. If you're comparing virtual care options for trauma-informed practice, it can help to compare telehealth tools for therapists before choosing how you want to receive support.
A therapy is useful when it moves a real goal forward. Less avoidance. Better sleep. More emotional control. Stronger relationships.
That is the standard that matters most.
Goal-Oriented Treatment at Casa Recovery
A treatment goal only helps if the program can support it. The level of care, the clinical structure, and the coordination between providers all affect whether a goal is realistic or just hopeful language on paper.
How level of care changes the pace of goal work
In a partial hospitalization setting, goals often focus on stabilization, routine, emotional containment, and reducing immediate impairment. In an intensive outpatient setting, people usually work on applying skills in real life while still receiving structured support. In standard outpatient therapy, goals often become more maintenance-focused, relational, and insight-driven.
That distinction matters because the same person may need different goals at different phases. Early on, the target may be attending treatment, sleeping more reliably, and reducing crisis behaviors. Later, the target may shift toward trust, identity, work functioning, or family repair.
A structured trauma program such as PTSD treatment in Southern California can give people access to multiple outpatient levels of care when weekly therapy alone is not enough structure.
Why integration changes outcomes
Trauma rarely fits neatly into one box. A person may need psychotherapy, psychiatric support, family involvement, and dual-diagnosis care at the same time. If those pieces are fragmented, goals often compete with each other. One provider works on sleep. Another works on trauma. Another addresses substance use. The client ends up holding the whole treatment system together alone.
An integrated program helps by aligning those moving parts. If medication is being adjusted, the therapist knows. If substance use is affecting trauma work, it becomes part of the plan instead of a side issue. If family dynamics are worsening symptoms, that gets addressed directly.
Effective program design is crucial. Small groups, frequent individual sessions, onsite psychiatry, family programming, and dual-diagnosis support are not extras. They make it easier to create goals that are practically workable in daily life.
Frequently Asked Questions About PTSD Treatment Goals
How long does it take to start feeling better
People often want an honest timeline, and they should. PTSD recovery is not instant, but meaningful change can begin earlier than many expect. One summary of recent clinical evidence reports that 46% of individuals improve within six weeks of beginning trauma-focused psychotherapy, and up to 40% recover within one year if they receive effective care, based on the data summarized by the WHO PTSD fact sheet.
That doesn't mean everyone follows the same path. Some people improve quickly in sleep, panic, or daily functioning before they notice deeper emotional change. Others move more slowly because they have dissociation, multiple traumas, or co-occurring conditions. Progress is still progress.
What if my first treatment does not work
This is one of the most painful fears people carry. If the first therapy doesn't help enough, many assume they are the problem. That is usually the wrong conclusion.
Some people don't respond well to the first approach they try. That doesn't mean recovery is over. It may mean the fit was wrong, the pace was wrong, or the person needed a different sequence of care. Emerging approaches for non-responders may include goals built around mindfulness toward vulnerable internal states, neurofeedback, or TMS, as discussed qualitatively in this review of PTSD treatment options beyond standard first-line care.
If one treatment falls short, the question is not “Why did I fail?” The better question is “What does this tell us about what I need next?”
Do treatment goals include family and work life
Yes. They should.
Many people measure recovery less by symptom language and more by life language. Can I keep a job? Can I be patient with my children? Can I stop withdrawing from my partner? Can I handle normal conflict without going into survival mode? Those are valid treatment goals, not side issues.
Family members also need guidance. Loved ones often help most when they learn what triggers flooding, how to respond to shutdowns, and how to support structure without becoming controlling.
What if I am not ready to talk about the trauma yet
That is common, and it does not mean treatment cannot begin. Some people need a phase of stabilization before direct trauma processing. The early goals may focus on sleep, emotional regulation, grounding, crisis reduction, and building trust with the therapist.
Starting there is not avoidance. It is preparation. Many people do better trauma work after they have reliable tools for staying present and safe enough inside their own body.
If you or someone you love needs structured trauma treatment with outpatient levels of care, family involvement, psychiatry, and dual-diagnosis support, Casa Recovery offers trauma-informed mental health programming in Southern California. The right treatment plan should feel clear, personalized, and doable. Reaching out for an assessment can help turn uncertainty into a practical next step.