Your phone is open to a dozen tabs. One says depression. Another says anxiety. Another says rehab, and that word alone makes your stomach drop.
Maybe you're looking for yourself. Maybe you're trying to help a son who stopped going to class, a partner who can't make it through work meetings anymore, or a parent who keeps saying they're “fine” while everything at home says otherwise. Weekly therapy hasn't been enough. But stepping away from life completely for residential treatment may feel impossible, too disruptive, or not like the right fit.
That in-between space is where many families get stuck.
A Mental Health Intensive Outpatient Program, often called a mental health IOP, is often the middle level of care people are trying to find when they say, “We need more help than this, but we're not sure we need hospitalization.” It offers structured treatment several days a week while allowing a person to keep living at home and stay connected to work, school, or family life when appropriate.
If you're also sorting through questions about technology and support tools, resources like Hyperleap AI's mental health solutions can help families understand how digital systems may support communication, navigation, and access in behavioral health settings. They don't replace treatment, but they can make a stressful search feel more manageable.
Table of Contents
- Introduction When Weekly Therapy Is Not Enough
- Deconstructing the Mental Health IOP Model
- Is an Intensive Outpatient Program Right for You
- Choosing Your Level of Care PHP vs IOP vs Outpatient
- A Look Inside a Typical IOP Week
- Navigating Insurance Costs and Scheduling
- How Casa Recovery Supports Your IOP Journey
Introduction When Weekly Therapy Is Not Enough
A lot of people arrive at a mental health IOP search after a slow build, not a single dramatic moment. Sleep gets worse. Panic starts showing up before work. Depression turns simple tasks into heavy lifts. Trauma symptoms keep breaking into the day. Someone is trying hard, showing up to therapy, taking medication, doing what they're supposed to do, and still slipping.
That doesn't mean they've failed treatment. It often means they need a different level of care.
A mental health IOP is built for that exact situation. It gives people more contact, more structure, and more therapeutic repetition than weekly outpatient therapy. But it doesn't require an overnight stay. For many families, that feels less frightening and more realistic. The person still sleeps in their own bed. They can often continue school, keep some work responsibilities, and practice new coping skills in real life instead of waiting until treatment ends.
The right question usually isn't “Is this bad enough?” It's “What amount of support matches what's happening right now?”
That shift matters. Families often delay care because they're trying to fit the crisis into the wrong category. They think the only options are “keep trying weekly therapy” or “go away to a hospital.” A mental health IOP sits in the middle. It offers coordinated treatment for people who are struggling in a serious way but don't need round-the-clock supervision.
You may also be reading because the situation isn't “just” depression or “just” anxiety. Maybe alcohol, cannabis, pills, or another substance has become part of how someone gets through the day. That creates even more confusion. Many families worry they'll be told to handle one problem first and then come back for the other later. In practice, good IOP care can address both together.
Deconstructing the Mental Health IOP Model
A mental health IOP is easiest to understand if you think of it as physical therapy for the mind and nervous system. You wouldn't expect one short appointment a week to rebuild strength after a major injury. You'd expect repetition, coaching, supervised practice, and a plan for using those skills at home. Mental health treatment works in a similar way when symptoms are disrupting life.
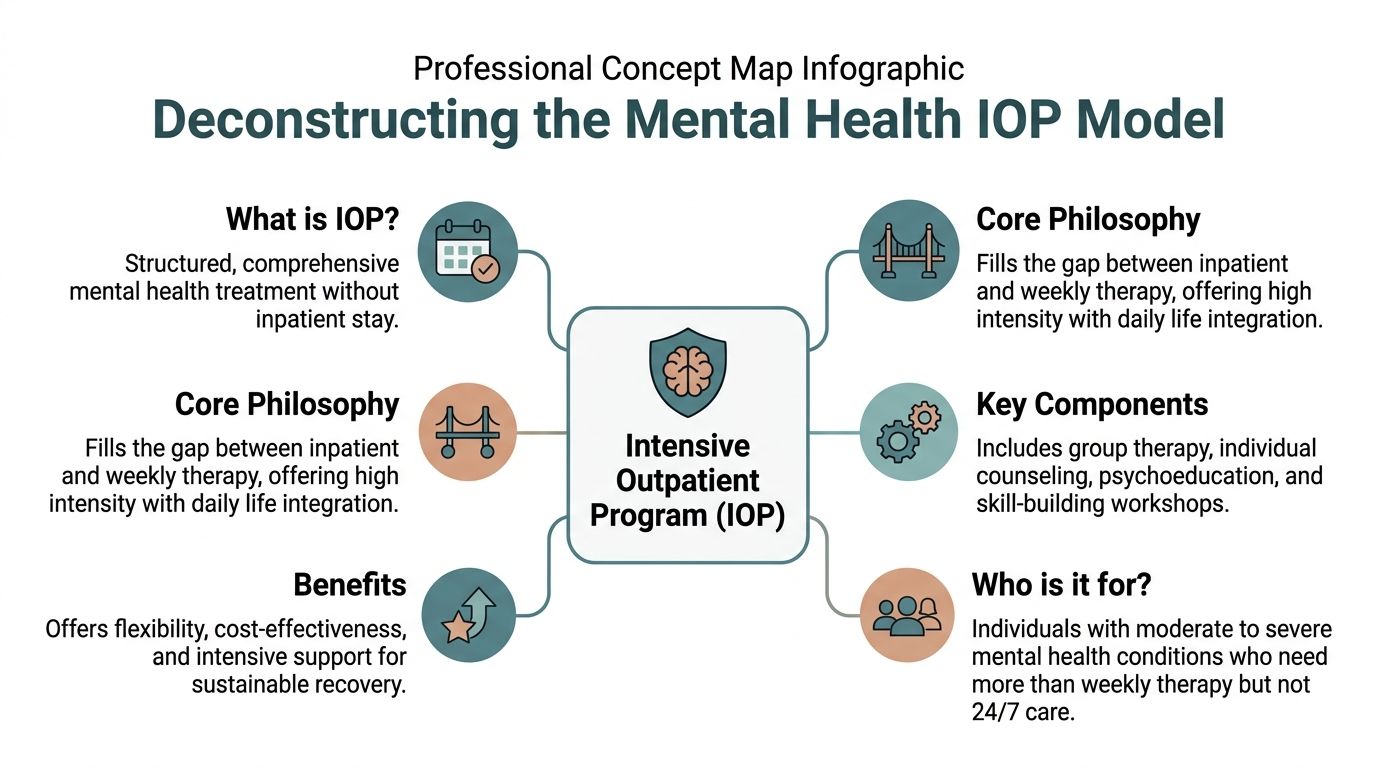
Why this level of care exists
IOP stands for Intensive Outpatient Program. “Outpatient” means you don't stay overnight. “Intensive” means care happens often enough to create traction.
Instead of one conversation every week or two, treatment is organized into a steady rhythm of therapy, skills work, and clinical oversight. In mental health settings, that often includes group therapy, individual sessions, psychoeducation, and psychiatric support. The person gets repeated chances to practice emotional regulation, communication, boundary-setting, relapse prevention, and other concrete skills while still living in their everyday environment.
That middle-ground design matters because many people need more than insight. They need containment and momentum. A mental health IOP can help when someone is too symptomatic for standard outpatient care but stable enough to remain at home.
Research on intensive outpatient treatment for substance use has found that IOPs show equivalent reductions in problem severity and increases in days abstinent compared to inpatient or residential care in randomized trials and quasi-experimental studies, according to the Journal of Substance Abuse Treatment review on intensive outpatient treatment. That doesn't mean every person should choose IOP over residential treatment. It means intensive outpatient care is a serious clinical option, not a watered-down one.
What treatment is trying to accomplish
A good program isn't just a place to vent. It has specific jobs to do.
- Stabilize symptoms: Help someone become less overwhelmed, less reactive, and more able to get through the day safely.
- Build repeatable skills: Teach tools that can be used between sessions, during conflict, at school, at work, and at home.
- Prevent backsliding: Catch patterns early. That can include mood decline, isolation, avoidance, self-harm urges, or substance use.
- Coordinate care: Keep therapists, psychiatry, and family support aligned instead of sending the person to disconnected providers.
Practical rule: If someone's life is narrowing because of their symptoms, more frequent care may be more useful than simply waiting longer for weekly therapy to work.
That structure is why many families feel relief once they understand what a mental health IOP is. It isn't a punishment. It isn't “rehab” in the vague way people often fear. It's organized treatment designed to help a person regain functioning while staying connected to ordinary life.
Is an Intensive Outpatient Program Right for You
Not everyone needs a mental health IOP. Some people do well with weekly therapy and medication management. Others need inpatient or residential care because safety is too unstable for outpatient treatment. IOP tends to fit the large middle group.
Signs daily life is being affected
A person may be a strong candidate when symptoms are no longer contained to private suffering and are starting to impair daily functioning.
You might notice things like:
- Work problems: missed shifts, reduced concentration, panic during meetings, or repeated call-outs
- School disruption: falling behind, avoiding class, or being too anxious or depressed to complete basic tasks
- Relationship strain: conflict at home, withdrawal from friends, or intense emotional swings that are hard to manage
- Loss of routine: sleeping all day, staying up all night, poor hygiene, isolation, or inability to keep appointments
- Escalating symptoms: worsening depression, anxiety, trauma reactions, emotional dysregulation, or repeated crises between therapy sessions
Someone can still be high-functioning on paper and need an IOP. Families often get confused here. A person may still have a job, still be enrolled in school, or still look composed in public. That doesn't mean they're coping well. What matters is how much effort it takes to hold things together and whether current support is enough.
If life outside treatment keeps falling apart between appointments, the treatment schedule may be too thin for the problem.
When mental health and substance use overlap
This is one of the most misunderstood parts of outpatient care.
Many people don't have a clean, single diagnosis. Anxiety may be tied to drinking. Depression may worsen after cannabis use. Trauma symptoms may lead someone to misuse medication or numb out with substances. Families often ask, “Do we treat the mental health issue first, or the substance use first?”
A more helpful answer is often both at the same time.
A 2025 University of Chicago Medicine article notes that IOPs are effective for “mental health symptoms accompanied by substance use” by integrating medication management and coping skills for both, which helps prevent fragmented care, as described in University of Chicago Medicine's discussion of when to consider intensive outpatient treatment.
That concurrent model matters in real life. If a person drinks to sleep because of panic, or uses substances after trauma triggers, separating treatment can miss the loop that's keeping everything going. In a dual-diagnosis IOP, clinicians can work on emotional regulation, psychiatric symptoms, medication questions, and substance-related coping in one coordinated plan.
Choosing Your Level of Care PHP vs IOP vs Outpatient
Most families don't struggle to decide whether they need help. They struggle to decide how much help fits.
The simplest way to sort this out is to compare the three most common non-residential options side by side.
| Feature | Traditional Outpatient | Intensive Outpatient (IOP) | Partial Hospitalization (PHP) |
|---|---|---|---|
| Time commitment | Usually one therapy or psychiatry appointment at a time | Multiple treatment sessions each week | Full-day structured programming on treatment days |
| Living situation | Live at home | Live at home | Live at home or in supportive housing |
| Best fit | Symptoms are distressing but manageable with periodic support | Symptoms are disrupting life and need more structure | Symptoms need near-daily clinical support without inpatient admission |
| Clinical focus | Ongoing maintenance, insight, medication follow-up | Stabilization, skill-building, accountability, coordinated care | Acute stabilization and step-down from hospital or residential care |
| Daily functioning | Person is generally functioning, though struggling | Person is functioning inconsistently or with increasing difficulty | Person often needs major support to get through the day safely |
| Flexibility | Highest flexibility | Moderate flexibility | Lowest flexibility among outpatient levels |
If you're trying to understand the distinction in more practical terms, this explanation of how IOP differs from PHP is useful because it frames the decision around intensity, structure, and who each level is designed to support.
A quick rule of thumb helps. Traditional outpatient works when progress is happening, even if slowly. PHP is often better when someone needs very frequent support and close monitoring. Mental health IOP often fits when a person needs substantial help but can still participate in life outside treatment.
The goal isn't to choose the “strongest” option. It's to choose the one that matches the person's current clinical picture.
A Look Inside a Typical IOP Week
The phrase “intensive outpatient” can sound intimidating until you see what a normal week looks like. In practice, the schedule is structured, but it isn't chaotic. It has rhythm.
Mental health IOPs typically involve 9 to 15 hours of structured clinical programming per week, delivered across three to five sessions, with common modalities including CBT and DBT, according to this overview of evidence-based therapy in intensive outpatient addiction treatment. That same source reports 60 to 70% success rates at six months post-discharge for mental health and dual-diagnosis IOPs.
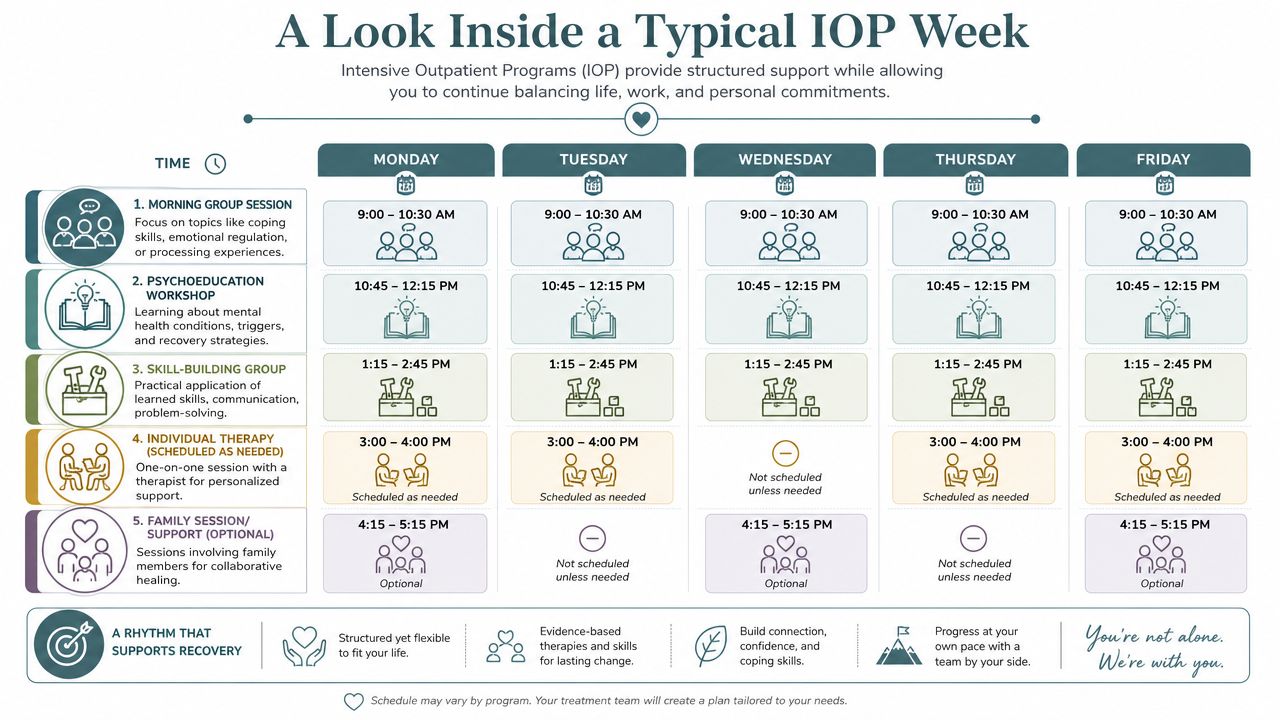
How the week is structured
A sample week often includes several types of care rather than the same thing repeated every day. If you'd like to visualize how that cadence can look, this sample weekly schedule for outpatient treatment gives a concrete sense of the flow.
Here's what that usually feels like from the client side:
- Group sessions on multiple days: These are often the backbone of IOP. People work on coping skills, emotional regulation, communication, relapse prevention, and processing current stressors with clinical guidance.
- Individual therapy: Individual therapy allows for personalized work. A therapist can connect group themes to trauma history, family dynamics, grief, identity concerns, or specific triggers.
- Psychiatric support: If medication is part of treatment, a psychiatrist or prescribing clinician can evaluate symptoms, monitor response, and make adjustments when needed.
- Psychoeducation: Clients learn how symptoms work. That might include the stress response, depression cycles, trauma triggers, or the link between thoughts, feelings, and behaviors.
- Family involvement when appropriate: Families may get education, communication guidance, or sessions that help reduce confusion and conflict at home.
What the therapies are for
Some therapy names sound technical, so it helps to translate them into plain language.
CBT, or Cognitive Behavioral Therapy, helps a person identify patterns in thinking and behavior that keep symptoms going. If someone instantly assumes failure, danger, or rejection, CBT gives them a way to challenge and reshape those patterns.
DBT, or Dialectical Behavior Therapy, is often useful when emotions feel intense, fast, or hard to control. It focuses on distress tolerance, emotional regulation, interpersonal effectiveness, and mindfulness.
Programs may also use trauma-focused approaches such as EMDR or Brainspotting, especially when trauma symptoms are driving panic, shutdown, dissociation, or self-protective behaviors. In a quality IOP, these tools aren't scattered randomly. The clinical team uses them as part of one treatment plan.
Group therapy isn't about being put on display. It's where many people stop feeling alone for the first time in months.
The structure helps because insight alone rarely changes behavior. Practice does. A mental health IOP gives people repeated chances each week to learn a skill, try it, talk about what happened, and refine it with support.
Navigating Insurance Costs and Scheduling
This is often the point where families pause. The clinical part may make sense, but then real life steps in. Can insurance cover it? How do you fit it around a job? What if someone is in school? What if calling the insurance company feels impossible right now?
Those concerns are normal. They also shouldn't stop someone from getting assessed.
What insurance usually wants to know
Insurance companies generally look for medical necessity. In plain language, that means the insurer wants documentation showing why this level of care is appropriate instead of a lower one. They may ask about symptom severity, functional impairment, recent treatment history, safety concerns, and whether weekly outpatient care has been enough.
Two terms come up often:
- Prior authorization: The insurer asks for clinical information before approving coverage, or before approving additional days.
- In-network and out-of-network benefits: An in-network provider has a contracted rate with the insurer. Out-of-network coverage may still exist, but the cost structure is different and usually needs to be verified carefully.
Medicare gives a useful benchmark for how insurers define this level of treatment. To be covered, an IOP must provide at least “9 hours of therapeutic services each week,” according to Medicare's coverage guidelines for outpatient intensive outpatient program services. Many private insurers use a similar threshold when evaluating medical necessity.
That detail matters because families often hear “flexible outpatient” and assume the time requirement is light. It isn't casual. It's a real commitment. But it's also not the same as stepping away from life entirely.
Insurance approval is often less about finding the right phrase and more about matching the clinical record to the correct level of care.
How people fit IOP into real life
Admissions teams prove especially helpful. A good admissions process doesn't just answer “Are you covered?” It helps answer “Can this work in our week?”
People in a mental health IOP often make practical adjustments like:
- Changing work hours temporarily: using leave, shifting to part-time, or moving to a later start
- Choosing evening or daytime tracks: depending on school, childcare, or job demands
- Reducing nonessential commitments: pausing clubs, social plans, or side projects so treatment has room to work
- Using virtual or hybrid options when appropriate: this can reduce commute stress, though the clinical fit still needs to be evaluated
Scheduling isn't just about math. It's about energy. A person may technically be able to work full time and attend IOP, but not every schedule is sustainable. Families do best when they plan for treatment to be a priority for a period of time, not something squeezed into leftover space.
If you're trying to understand how coverage and outpatient mental health benefits may apply in a real Orange County setting, this overview of mental health outpatient and IOP coverage through Blue Shield can help clarify the kinds of questions to ask during verification.
A strong admissions team usually handles benefit checks, explains deductible and authorization issues in plain English, and works with the family to map out a realistic attendance plan. That support matters because people don't seek care at their most organized moment. They seek care when things are already hard.
How Casa Recovery Supports Your IOP Journey
When a provider offers mental health IOP care well, families can feel the difference quickly. Calls are returned. Questions get answered clearly. The program doesn't act confused by trauma, substance use, medication needs, or family stress. It expects those layers and knows how to work with them.
What quality outpatient care looks like
Casa Recovery provides outpatient mental health and dual-diagnosis treatment in Orange County with several features families often need but don't always know to ask about.
Those include:
- Trauma-informed treatment: useful when depression, anxiety, emotional dysregulation, or substance use is tied to unresolved trauma
- Integrated psychiatry onsite: medication evaluation and management are part of the treatment environment instead of being split off elsewhere
- Small groups and a high therapist-to-client ratio: this supports more individualized attention
- Concurrent dual-diagnosis care: mental health symptoms and substance use concerns are addressed together rather than in separate tracks
- A formal family program: education, therapy, and communication support help the whole household move in the same direction
That combination matters because outpatient treatment can break down when it becomes fragmented. One provider handles medication. Another handles therapy. A third focuses on substance use. The family is left trying to connect the dots. A more integrated model reduces that burden.
Why operational support matters too
Families usually focus on clinicians first, and that's appropriate. But operations shape the treatment experience too. Insurance verification, benefit coordination, scheduling, and communication systems affect whether someone gets into care smoothly or gives up halfway through the intake process.
For organizations and readers who want a better understanding of the billing and administrative side behind access to care, effective mental health RCM strategies can shed light on why front-end insurance and revenue cycle processes matter so much in behavioral health.
A strong provider doesn't make you chase every answer yourself. It helps translate a crisis into the next doable step.
If you or someone you love may need structured outpatient support, Casa Recovery offers confidential admissions guidance, insurance verification, and help determining whether PHP, IOP, or another level of care fits best. If you're in Orange County, Los Angeles, San Diego, or coming from out of area, reaching out for a conversation can turn a very overwhelming situation into a clear plan.