You may be trying to answer a simple question and finding that every treatment program sounds the same. The website says evidence-based. The admissions call says individualized. The brochure mentions trauma-informed care, psychiatry, family support, and life skills. For families and referring professionals, the hard part isn't finding options. It's separating real clinical quality from polished language.
That distinction matters most in outpatient treatment, especially in PHP and IOP settings where people are trying to stabilize symptoms, rebuild daily functioning, and avoid another level of care. A strong program doesn't just offer therapy names. It translates clinical best practices into day-to-day operations, staffing choices, measurement, and coordinated follow-through.
The most reliable way to judge quality is to ask how a program makes decisions. What treatment model guides care. How progress is tracked. How psychiatry and therapy work together. What happens when a client isn't improving. Those questions reveal far more than a generic promise of compassionate support.
Table of Contents
- Navigating the Search for Quality Mental Health Care
- What Are Clinical Best Practices in Mental Health
- Core Evidence-Based Therapies Explained
- Implementing Best Practices in Outpatient Programs
- The Pillars of Integrated and Continuous Care
- Measuring Quality and Ensuring Accountability
- Finding Clinical Best Practices in Orange County
Navigating the Search for Quality Mental Health Care
A family may call after an ER visit, a failed college semester, or a relapse that followed what looked like a stable month. A referring therapist may know the client needs more structure, but still have to sort through programs that all claim to offer evidence-based care. The hard part is not finding treatment options. The hard part is judging which program can translate good clinical theory into day-to-day care that is effective.
That is where "clinical best practices" becomes useful in a practical sense. It gives families and referring professionals a way to evaluate how a program operates, not just how it describes itself on a website.
What informed evaluation sounds like
The most useful questions are operational.
- How do you choose therapies: Do clinicians match treatment to the client's presentation, risk profile, and functional needs, or does everyone enter the same template?
- How often do clients meet individually: Group work can build skills and reduce isolation, but some clients also need recurring individual sessions to process trauma, clarify goals, and address avoidance or ambivalence.
- Is psychiatry integrated: Medication management works better when prescribers, therapists, and case managers are coordinating in real time.
- How do you know treatment is working: A strong program can explain what it measures, how often it reviews progress, and what changes when someone stalls or declines.
- What does step-down planning look like: Good outpatient care includes relapse planning, family communication when appropriate, and a clear handoff to the next level of support.
In my experience, strong programs answer these questions plainly. They can explain why a client is in PHP rather than IOP, why one modality was selected over another, and what would trigger a revision to the treatment plan.
What often goes wrong
The gap is usually in execution. Many programs can list CBT, DBT, trauma-informed care, and dual-diagnosis treatment. Fewer can explain who is trained to deliver each intervention, how treatment teams coordinate across disciplines, how supervision protects quality, and how outcomes are reviewed often enough to change care before a client drifts off course.
That distinction matters in PHP and IOP, where clients are stable enough to remain in the community but still need a high level of structure, monitoring, and clinical coordination. In dual-diagnosis care, the standard should be integrated treatment rather than parallel tracks for mental health and substance use. SAMHSA's guidance on co-occurring disorders makes that point clearly in its overview of integrated treatment for co-occurring disorders.
Strong programs also build systems around clinical judgment. That includes staffing patterns, case review, family communication protocols, and outcome tracking. The same implementation principle shows up in other healthcare fields. OMOPHub on healthcare LLM best practices describes a similar issue. Quality depends on how a model is grounded, monitored, and used in practice, not just on whether the right concept appears in a brochure.
Clinical best practices give families and referral partners a better filter. They point attention to the program's actual treatment process, which is where quality is either proven or exposed.
What Are Clinical Best Practices in Mental Health
The shortest useful definition is this: clinical best practices combine strong research, clinician judgment, and the client's actual needs and values. If one of those pieces is missing, treatment gets weaker.
That model is often described as a three-legged stool. Remove one leg and the whole thing becomes unstable. Research alone isn't enough if the clinician can't apply it well. Experience alone isn't enough if the method has never been properly tested. A treatment plan that ignores the client's culture, goals, or preferences may be technically correct and still fail in practice.
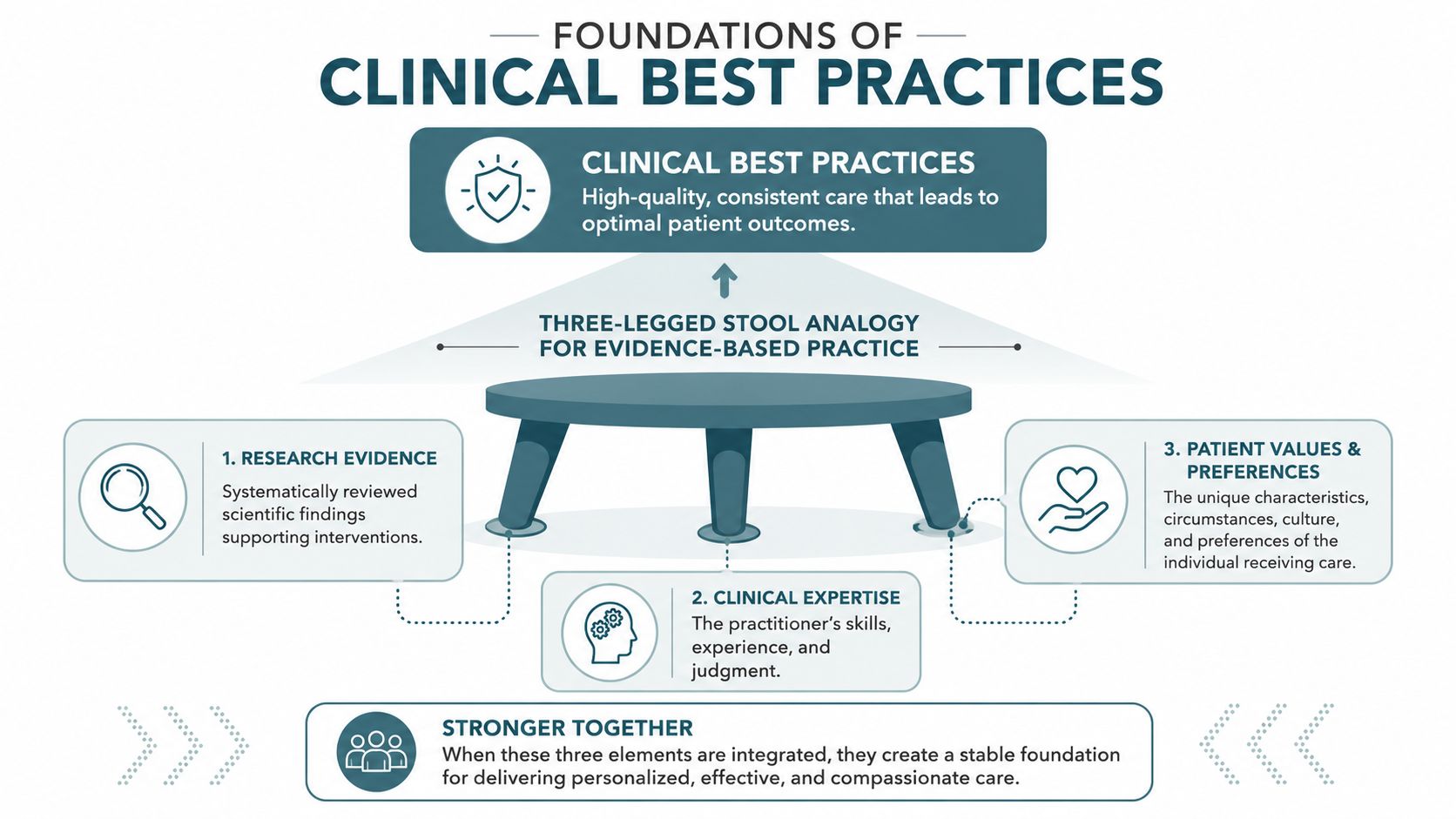
Evidence-based practice integrates the latest scientific research, the clinician's professional experience and judgment, and the patient's values, preferences, and cultural context. A therapeutic intervention is classified as an empirically supported treatment when it has been validated by at least two rigorous randomized controlled trials (NMVVRC overview of evidence-based treatments and practices).
Why evidence matters in real treatment decisions
This isn't about turning therapy into a script. It's about reducing guesswork. Treatments grounded in evidence-based practice are different from approaches built mainly on theory, intuition, or tradition. The field has many ideas that sound convincing. Fewer have been tested rigorously enough to earn the status of an empirically supported treatment.
That distinction helps families and referring professionals cut through marketing language. If a program says it uses CBT, DBT, or EMDR, the next question should be whether those interventions are delivered within an evidence-based framework and adapted to the individual sitting in the room.
A similar principle applies outside direct patient care. In health technology, for example, teams working with AI systems increasingly emphasize grounding, verification, and reliable clinical context rather than plausible-sounding output. OMOPHub on healthcare LLM best practices is a useful example of that broader discipline of evidence-aware implementation.
What separates a strong program from a persuasive one
A persuasive program tells you it cares. A strong program shows you how care is organized.
Look for signs that treatment decisions are made deliberately:
- Validated methods: The core modalities should come from approaches with empirical support, not just branded in-house concepts.
- Clinical discretion: Skilled clinicians should be able to adjust pacing, sequencing, and emphasis based on presentation.
- Client fit: Treatment should account for history, motivation, culture, functioning, and readiness, rather than forcing everyone through the same template.
When those three parts are integrated, "best practices" becomes concrete. It shapes the treatment plan, the therapeutic relationship, and the odds that care will help.
Core Evidence-Based Therapies Explained
Families often hear a string of acronyms and assume they all mean the same thing. They don't. Each therapy is designed to solve a different clinical problem. Good outpatient treatment doesn't pick a favorite and use it for everyone. It matches the intervention to the obstacle in front of the client.
How these therapies solve different problems
CBT is often the clearest starting point. It helps clients identify patterns in thinking and behavior that keep symptoms in place. For depression, that may mean challenging hopeless conclusions and re-engaging with life. For anxiety, it often means testing fearful predictions instead of obeying them.
DBT is different. It focuses on emotion regulation, distress tolerance, interpersonal effectiveness, and mindfulness. It's useful when someone's problem isn't just what they think, but how fast they become overwhelmed and how difficult it is to stay steady when intense emotion hits.
EMDR is built for trauma processing. It helps people work through distressing memories that continue to drive present-day symptoms. When trauma is central, supportive talk therapy alone often isn't enough.
Brainspotting is also used in trauma-focused work. In practice, clinicians may use it when a client has difficulty accessing or verbalizing material directly, or when body-based activation is prominent and standard cognitive approaches aren't reaching the issue fully.
For clients with both mental health and substance use concerns, integrated dual-diagnosis treatment matters because sequential care often fails. Treating anxiety now and substance use later, or vice versa, can leave each problem feeding the other.
A strong motivational style also matters in this population. For readers who want a plain-language overview of one engagement method used in dual-diagnosis settings, Still Water Wellness MI treatment offers a useful explanation of motivational interviewing and why it can help clients move from resistance to participation.
Comparing modalities side by side
| Modality | Primary Focus | Best For Treating |
|---|---|---|
| CBT | Restructuring unhelpful thoughts and behaviors | Depression, anxiety, avoidance patterns, relapse-triggering thought cycles |
| DBT | Building practical skills for managing intense emotions | Emotional dysregulation, impulsivity, conflict, self-defeating coping |
| EMDR | Processing traumatic memories that remain emotionally charged | Trauma, PTSD symptoms, intrusive recall, persistent triggers |
| Brainspotting | Accessing and processing trauma through focused attention and body awareness | Trauma-related activation, hard-to-verbalize distress, somatic intensity |
| Integrated Dual-Diagnosis Treatment | Treating mental health and substance use together in one plan | Co-occurring disorders where each condition worsens the other |
The right question isn't "Which therapy is best?" It's "Which therapy fits the client's primary barriers right now?"
Some programs do offer several of these modalities under one roof. One example is Casa Recovery's evidence-based mental health approaches, which lists therapies such as CBT, DBT, EMDR, Brainspotting, and motivational interviewing within an outpatient framework. The important issue isn't the menu by itself. It's whether the program knows when and how to use each option.
Implementing Best Practices in Outpatient Programs
A treatment philosophy only matters if the program can deliver it consistently. In PHP and IOP care, implementation lives in the schedule, staffing pattern, supervision, and daily environment. That's where clinical best practices either become real or fall apart.

Staffing shapes the treatment experience
High-quality outpatient care usually depends on enough clinicians being available to do more than manage a schedule. Clients need timely individual sessions, thoughtful group facilitation, and case coordination that doesn't get squeezed out by volume.
Small groups matter because they change what can happen in the room. Clients speak more, receive more feedback, and become less likely to disappear into the background. A high therapist-to-client ratio also gives staff more room to notice early warning signs such as shutdown, agitation, disengagement, or escalating relapse risk.
Training is another operational marker. Programs that take best practices seriously don't assume a license alone is enough. They invest in ongoing instruction, supervision, and calibration so that evidence-based therapies are delivered competently rather than loosely imitated.
Trauma-informed care has to be operational
Trauma-informed care isn't a slogan for the website. It should shape intake, group norms, crisis response, boundaries, pacing, and the way staff speak with clients when symptoms spike.
That often means practical choices such as:
- Predictable structure: Clients know what the day will look like and what is expected of them.
- Choice where possible: Staff offer appropriate options instead of using unnecessary power struggles.
- Interdisciplinary coordination: Therapists, psychiatric providers, case managers, and support staff share information and work from the same formulation.
- Attention to safety: Emotional safety is treated as a clinical condition, not an optional extra.
Emerging research found that 74% of patients in dual-diagnosis outpatient tracks reported feeling "judgment-free" only when providers used interdisciplinary teams, which highlights how staffing and trauma-informed design affect the client's experience of care (University of New Mexico community toolkit overview).
For families comparing levels of care, it also helps to review what a structured program includes. Casa Recovery's mental health IOP is one example of how outpatient treatment can be organized around repeated contact, small-group work, and ongoing clinical support rather than occasional therapy alone.
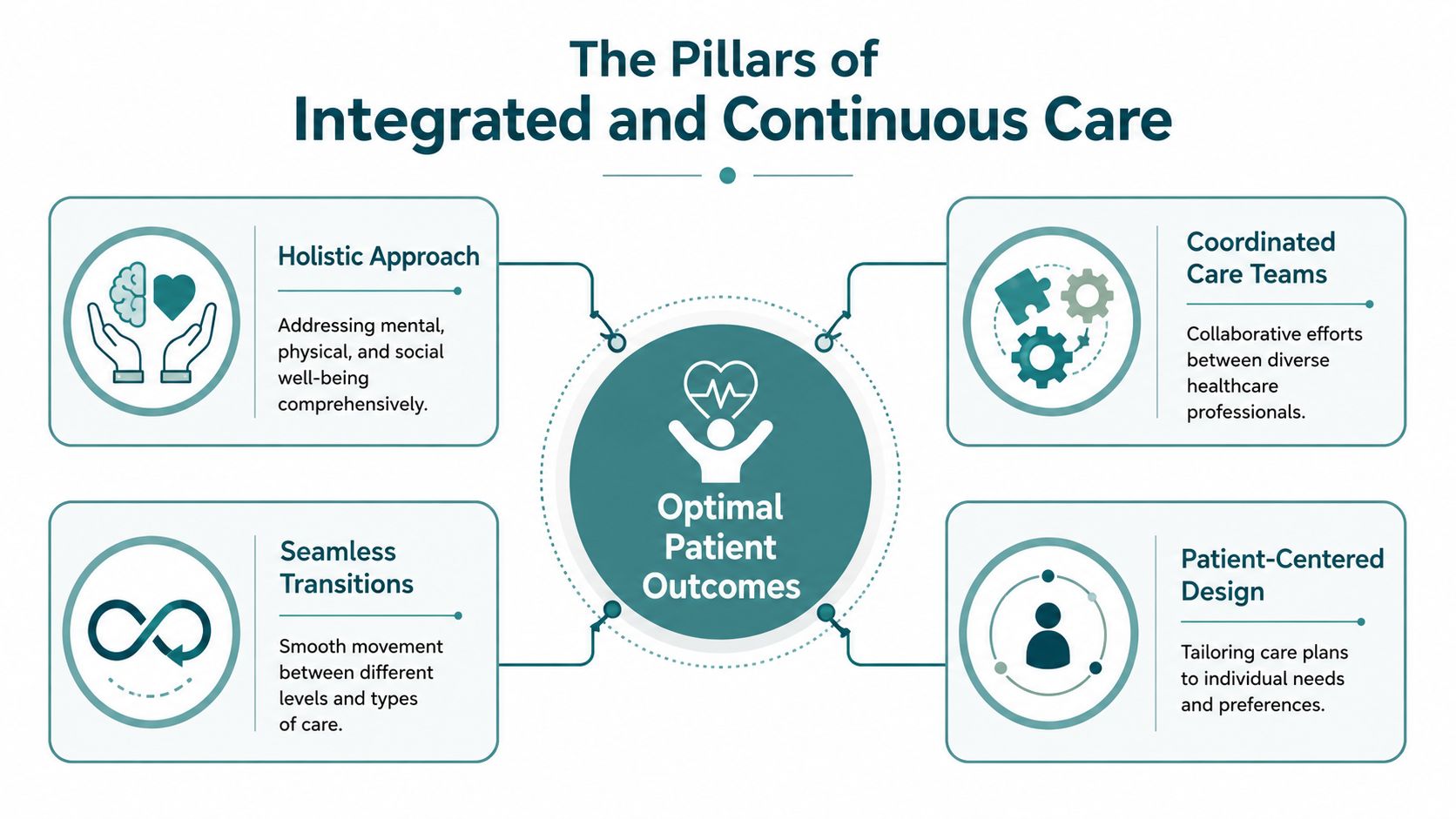
The Pillars of Integrated and Continuous Care
People usually don't struggle because one isolated symptom appeared in one isolated setting. Mood instability affects sleep, work, and family conflict. Substance use complicates psychiatric symptoms. Medication issues can make therapy harder. Housing instability can undermine even strong clinical work. That's why fragmented care often produces fragile progress.
Why fragmentation undermines progress
When psychotherapy, psychiatry, family communication, and recovery planning happen in separate silos, each provider sees only part of the picture. The therapist may not know a medication changed. The prescriber may not hear about relapse triggers emerging in group. The family may unintentionally reinforce the very patterns treatment is trying to change.
Evidence-based systems respond to that problem with stepped-care, meaning treatment intensity is adjusted according to patient response. This model is associated with improved retention and reduced psychiatric hospitalization. The same evidence base also supports combining Medication Support Services with behavioral therapies for many complex disorders (USPSTF methods for evidence-based behavioral counseling approaches).
What continuity looks like in practice
In a strong outpatient program, continuity usually rests on a few concrete pillars:
- Family involvement: A formal family program helps relatives understand symptoms, boundaries, communication patterns, and relapse risks. It also reduces the common problem of everyone reacting to the crisis differently.
- Onsite psychiatry: When psychiatric evaluation and medication management are integrated into the same treatment setting, clinicians can align prescribing decisions with observed behavior, therapy goals, and client feedback.
- Supportive transitions: Some clients need coordination with supportive living, outpatient therapists, recovery resources, or other community supports so discharge doesn't become a cliff.
- One treatment story: The client shouldn't have to stitch together separate explanations from separate providers.
Care becomes more effective when everyone treating the client is working from the same formulation, not just the same calendar.
For clinicians and families evaluating integrated systems, Casa Recovery's integrated treatment approach illustrates how mental health and substance use treatment can be coordinated concurrently rather than treated as separate episodes of care.
Measuring Quality and Ensuring Accountability
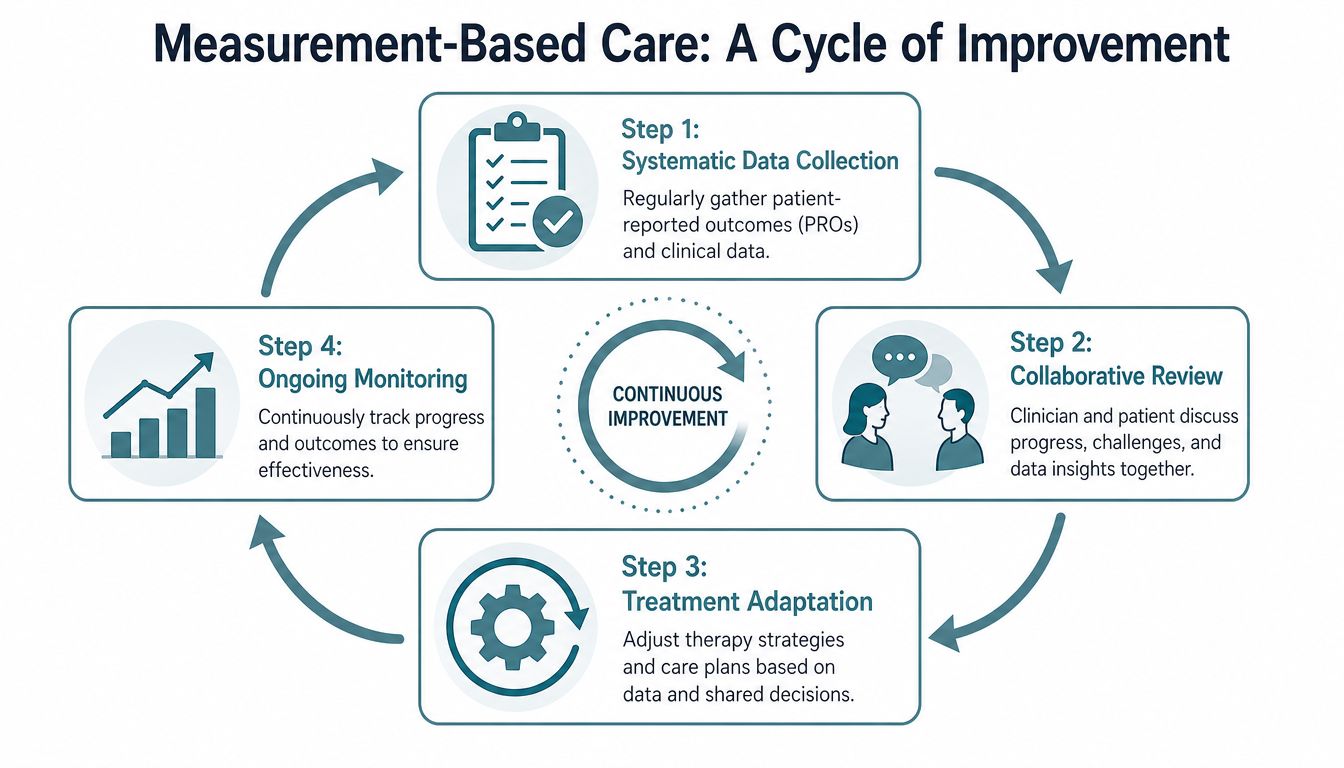
A program can sound thoughtful and still miss the mark clinically. The difference between confidence and accountability is measurement. In mental health care, that means tracking symptoms and response in a structured way instead of relying only on impressions.
Measurement changes clinical decisions
Measurement-Based Care uses standardized tools to monitor progress over time. In practice, that often includes measures such as the PHQ-9 for depression and the GAD-7 for anxiety, administered regularly rather than only at intake.
That matters because symptom drift is easy to miss in ordinary conversation. A client may say they are "doing okay" while depression is worsening, sleep is collapsing, or anxiety is steadily narrowing daily functioning. A structured measure gives the team a common reference point and creates a reason to revisit the treatment plan early.
According to the American Psychological Association's policy guidance, when psychologists actively monitor patient progress using standardized tools, it is associated with a significant reduction in deterioration rates, and this kind of monitoring acts as a safety net by identifying problematic treatment response early (APA policy on psychological practice in health care).
Accountability also includes data handling
Measurement isn't only about collecting scores. The team has to review the results, discuss them with the client, and make changes when the data and the lived experience don't line up.
That process usually looks like this:
- Collect data regularly: Not just when there's a crisis.
- Review trends clinically: A score means little without interpretation.
- Adjust treatment deliberately: Increase support, change modality, revisit diagnosis, or coordinate psychiatry when needed.
- Repeat the cycle: Good care is iterative.
Programs also need to handle this information responsibly. Families and referring professionals increasingly ask how outcome data, documentation, and sensitive records are stored and shared. For a practical overview of broader operational concerns, protecting client data guidelines is a useful resource on data security and compliance principles that matter whenever confidential health information is involved.
If a program says it individualizes care, it should also be able to show how it detects when the current plan isn't working.
Finding Clinical Best Practices in Orange County
A common Orange County referral starts with pressure. A therapist sees symptoms accelerating and recommends PHP. A hospital discharge planner needs a step-down option within days. A family has tried weekly outpatient care and can see it is no longer enough. In that moment, the question is not whether a program sounds credible on a website. The question is whether the program can assess accurately, start treatment quickly, and keep care organized across therapy, psychiatry, family work, and aftercare.
That is where the difference between academic best practices and real outpatient execution becomes clear. A high-quality PHP or IOP does more than name evidence-based therapies. It shows how those methods are staffed, coordinated, and adjusted when a client is not improving.
A practical checklist for evaluating programs
Ask direct questions. Strong programs answer them clearly and specifically.
- How is the treatment plan built? Ask how the team decides which therapies fit the client's diagnosis, risks, stage of change, and daily functioning.
- Who is on the treatment team? Ask whether therapists, psychiatry, case management, and family clinicians work from one shared plan or operate in parallel.
- How are mental health and substance use treated together? Dual-diagnosis care should be integrated in the same program, not split into separate tracks that compete for attention.
- What does trauma-informed care look like day to day? Listen for specifics such as group pacing, staff training, crisis response, and how the program avoids recreating instability or shame.
- How often is progress reviewed? Good programs use structured measures, clinical observation, and client feedback, then change the plan when the current approach is falling short.
- What happens at transitions? Ask who coordinates the handoff to lower levels of care, outpatient providers, sober supports, or family systems after PHP or IOP ends.
In practice, these questions matter because Orange County has no shortage of programs. The harder task is finding one that can translate a strong clinical model into consistent daily care.
Local context matters too. Orange County Health Care Agency reporting shows ongoing demand for behavioral health and substance use services across the county, especially during periods of acute need and care transition (Orange County Health Care Agency behavioral health services). That does not tell you which program is right for a specific client, but it does explain why rushed placements happen and why referral sources need to ask sharper operational questions.
The best referral conversations stay concrete. Ask how the team handles a client whose depression, trauma symptoms, and alcohol use are feeding each other. Ask how medication decisions are communicated to primary therapists and families. Ask what the program does in week two if attendance drops, sleep worsens, or group participation collapses.
Programs that practice well usually answer in plain language. They can explain staffing ratios, psychiatric access, family contact, crisis procedures, and discharge planning without hiding behind broad claims.
If you're looking for structured outpatient mental health or dual-diagnosis care in Orange County, Casa Recovery provides PHP and IOP services with integrated psychiatry, trauma-informed programming, evidence-based therapies, and family support. For families and referring professionals, the useful comparison is simple. Look at whether the program's daily operations match the clinical standards it describes.